

MRI-Based Pancreatic Atrophy Is Associated With Malignancy or Invasive Carcinoma in Intraductal Papillary Mucinous Neoplasm
- PMID: 35719938
- PMCID: PMC9204001
- DOI: 10.3389/fonc.2022.894023
MRI-Based Pancreatic Atrophy Is Associated With Malignancy or Invasive Carcinoma in Intraductal Papillary Mucinous Neoplasm
Abstract
Background: Abrupt change in the caliber of the main pancreatic duct (MPD) with distal pancreatic atrophy (PA) was considered as one of worrisome features in the International Association of Pancreatology guideline and American College of Gastroenterology guideline for the management of intraductal papillary mucinous neoplasms (IPMNs). However, this feature was not included in other guidelines. Moreover, the association between PA alone and malignancy in IPMNs has not been fully evaluated. In the present study, we investigated the role of image-based PA in identifying malignant IPMNs or invasive carcinoma.
Methods: A total of 186 patients with IPMNs were included for analysis. The tumor size, location, MPD diameter, presence of a mural nodule (MN), and PA were evaluated using magnetic resonance imaging. Demographic information and serum carbohydrate antigen 19-9 and carcinoembryonic antigen (CEA) levels were also collected. IPMNs with high-grade dysplasia and associated invasive carcinoma were regarded as malignant IPMNs.
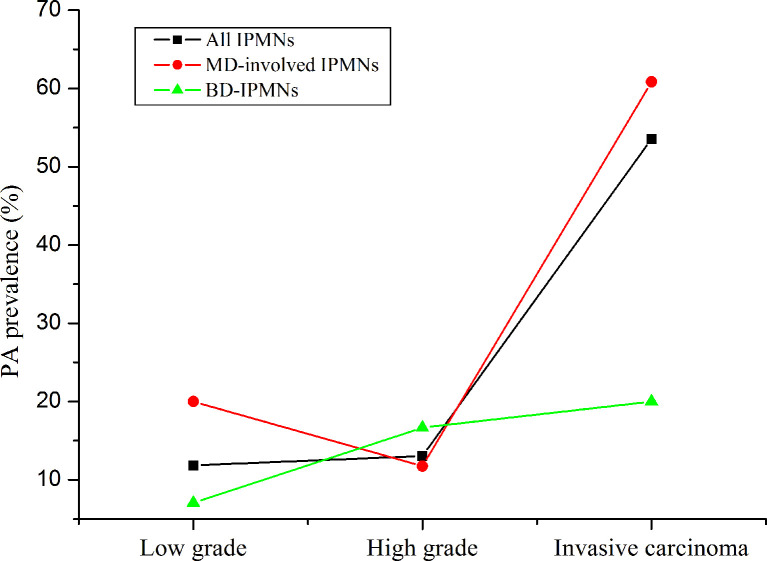
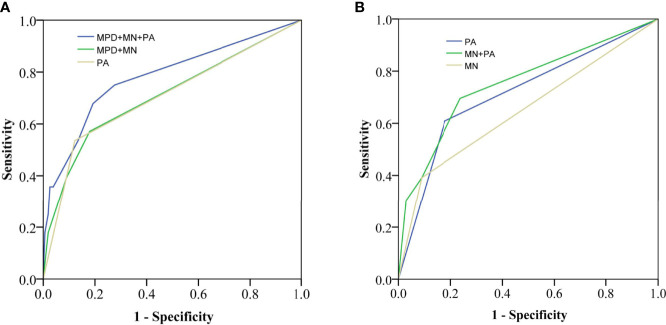
Results: PA was observed in 34 cases (18.3%). The occurrence of malignant IPMNs or invasive carcinoma in patients with PA were significantly higher than in those without PA (52.9% vs. 22.3%; 44.1% vs. 8.9%, all P < 0.01). Multivariate logistic regression analysis showed that PA was an independently associated factor for malignant IPMNs [odds ratio (OR) = 2.69, 95% confidence interval (CI): 1.07-6.78] or invasive carcinoma (OR = 7.78, 95%CI: 2.62-23.10) after modified with confounders. Subgroup analysis in MPD-involved IPMNs also indicated that PA was an independently associated factor for invasive carcinoma (OR = 9.72, 95%CI: 2.43-38.88). PA had a similar performance with MPD plus MN [the area under the curve (AUC) was both 0.71] in identifying malignancy. PA had a higher performance in identifying invasive carcinoma in MPD-involved IPMNs than MN (AUC = 0.71 vs. 0.65, P = 0.02).
Conclusion: Our data showed that imaging-based PA was associated with malignancy or invasive carcinoma regardless of abrupt change in the caliber of MPD in IPMNs. PA had an acceptable performance in identifying malignant IPMNs.
Keywords: intraductal papillary mucinous neoplasms; invasive carcinoma; malignancy; pancreas; pancreatic atrophy.
Copyright © 2022 Lin, Chen, Liu, Cao, Cui, Wang, Wang and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Threshold of main pancreatic duct for malignancy in intraductal papillary mucinous neoplasm at head-neck and body-tail.BMC Gastroenterol. 2022 Nov 19;22(1):473. doi: 10.1186/s12876-022-02577-3. BMC Gastroenterol. 2022. PMID: 36402960 Free PMC article.
-
Threshold of Main Pancreatic Duct Diameter in Identifying Malignant Intraductal Papillary Mucinous Neoplasm by Magnetic Resonance Imaging.Technol Cancer Res Treat. 2023 Jan-Dec;22:15330338231170942. doi: 10.1177/15330338231170942. Technol Cancer Res Treat. 2023. PMID: 37078135 Free PMC article.
-
The association between serum ferritin levels and malignant intraductal papillary mucinous neoplasms.BMC Cancer. 2021 Nov 20;21(1):1253. doi: 10.1186/s12885-021-08986-z. BMC Cancer. 2021. PMID: 34800987 Free PMC article.
-
Cyst features and risk of malignancy in intraductal papillary mucinous neoplasms of the pancreas: a meta-analysis.Clin Gastroenterol Hepatol. 2013 Aug;11(8):913-21; quiz e59-60. doi: 10.1016/j.cgh.2013.02.010. Epub 2013 Feb 13. Clin Gastroenterol Hepatol. 2013. PMID: 23416279 Review.
-
Ductal Dilatation of ≥5 mm in Intraductal Papillary Mucinous Neoplasm Should Trigger the Consideration for Pancreatectomy: A Meta-Analysis and Systematic Review of Resected Cases.Cancers (Basel). 2021 Apr 22;13(9):2031. doi: 10.3390/cancers13092031. Cancers (Basel). 2021. PMID: 33922344 Free PMC article. Review.
Cited by
-
Navigating Intraductal Papillary Mucinous Neoplasm Management through Fukuoka Consensus vs. European Evidence-Based Guidelines on Pancreatic Cystic Neoplasms-A Study on Two European Centers.Cancers (Basel). 2024 Jun 6;16(11):2156. doi: 10.3390/cancers16112156. Cancers (Basel). 2024. PMID: 38893274 Free PMC article.
-
Modern aspects of the management of pancreatic intraductal papillary mucinous neoplasms: a narrative review.Rom J Morphol Embryol. 2022 Jul-Sep;63(3):491-502. doi: 10.47162/RJME.63.3.03. Rom J Morphol Embryol. 2022. PMID: 36588487 Free PMC article. Review.
-
Early features of pancreatic cancer on magnetic resonance imaging (MRI): a case-control study.Abdom Radiol (NY). 2024 May;49(5):1489-1501. doi: 10.1007/s00261-024-04271-2. Epub 2024 Apr 5. Abdom Radiol (NY). 2024. PMID: 38580790
References
LinkOut - more resources
Full Text Sources