

Comprehensive Analyses of Ferroptosis-Related Alterations and Their Prognostic Significance in Glioblastoma
- PMID: 35720126
- PMCID: PMC9204216
- DOI: 10.3389/fmolb.2022.904098
Comprehensive Analyses of Ferroptosis-Related Alterations and Their Prognostic Significance in Glioblastoma
Abstract
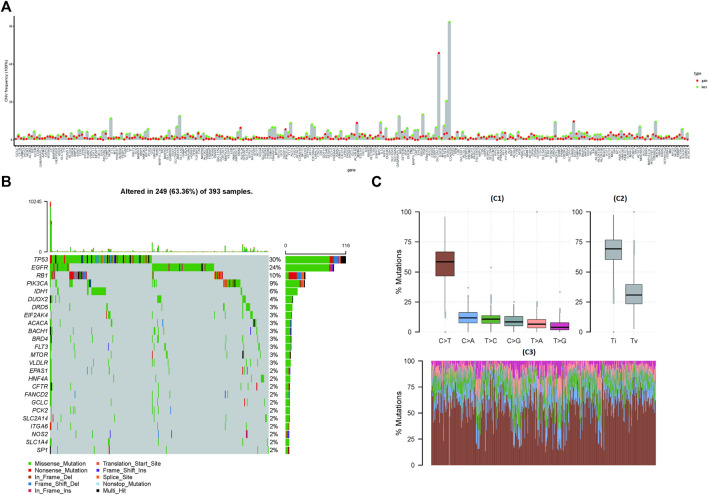
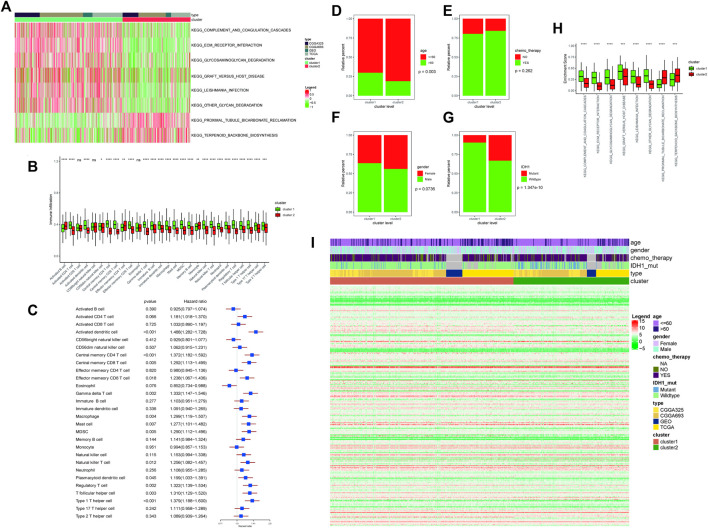
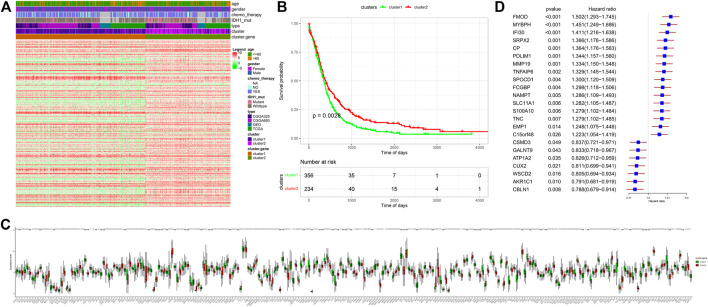
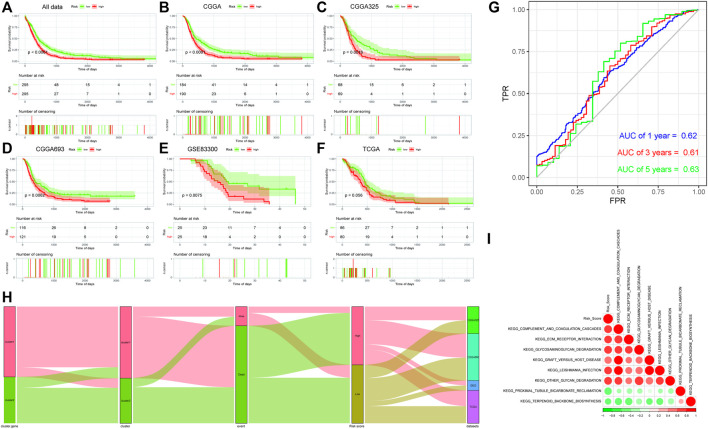
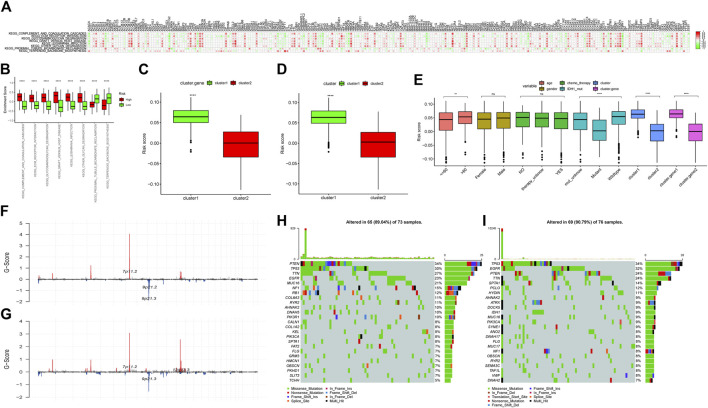
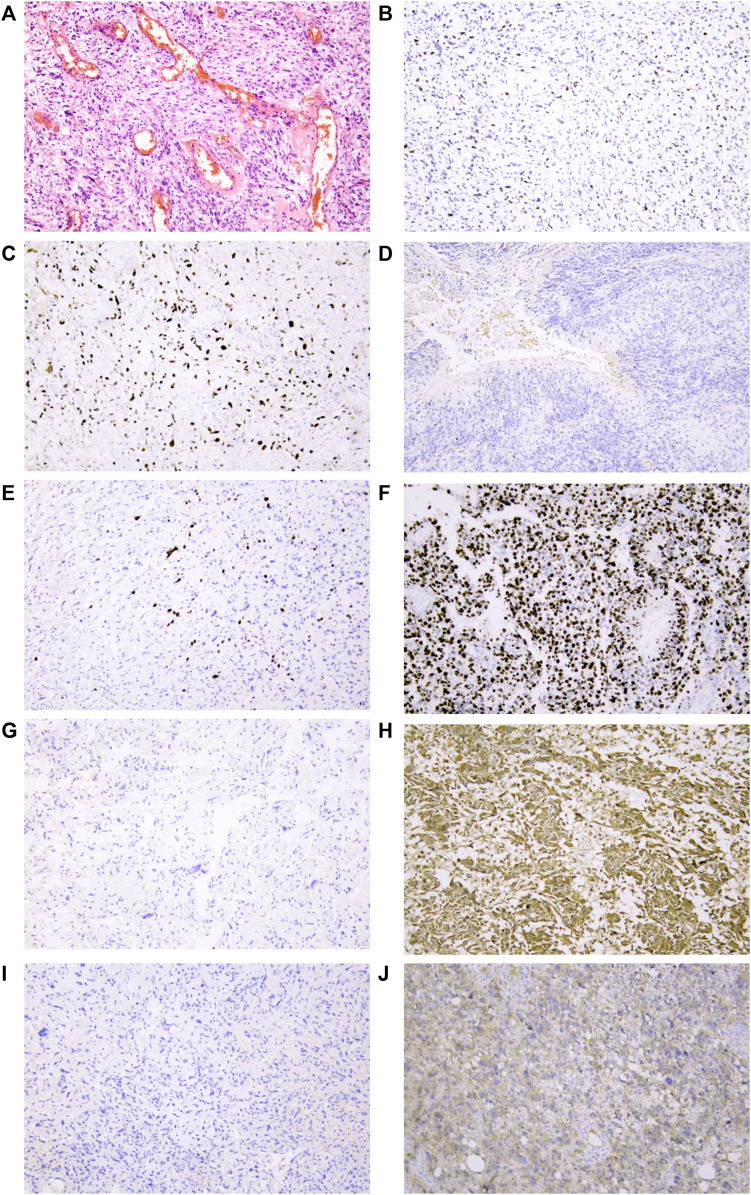
Background: This study was designed to explore the implications of ferroptosis-related alterations in glioblastoma patients. Method: After obtaining the data sets CGGA325, CGGA623, TCGA-GBM, and GSE83300 online, extensive analysis and mutual verification were performed using R language-based analytic technology, followed by further immunohistochemistry staining verification utilizing clinical pathological tissues. Results: The analysis revealed a substantial difference in the expression of ferroptosis-related genes between malignant and paracancerous samples, which was compatible with immunohistochemistry staining results from clinicopathological samples. Three distinct clustering studies were run sequentially on these data. All of the findings were consistent and had a high prediction value for glioblastoma. Then, the risk score predicting model containing 23 genes (CP, EMP1, AKR1C1, FMOD, MYBPH, IFI30, SRPX2, PDLIM1, MMP19, SPOCD1, FCGBP, NAMPT, SLC11A1, S100A10, TNC, CSMD3, ATP1A2, CUX2, GALNT9, TNFAIP6, C15orf48, WSCD2, and CBLN1) on the basis of "Ferroptosis.gene.cluster" was constructed. In the subsequent correlation analysis of clinical characteristics, tumor mutation burden, HRD, neoantigen burden and chromosomal instability, mRNAsi, TIDE, and GDSC, all the results indicated that the risk score model might have a better predictive efficiency. Conclusion: In glioblastoma, there were a large number of abnormal ferroptosis-related alterations, which were significant for the prognosis of patients. The risk score-predicting model integrating 23 genes would have a higher predictive value.
Keywords: alterations; ferroptosis; glioblastoma; predictive models; prognosis.
Copyright © 2022 Tian, Liu, Zhang, Liu, Wu, Yang, Zhao and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Ferroptosis related genes are regulated by methylation and predict the prognosis of glioblastoma patients.Transl Cancer Res. 2022 Apr;11(4):603-614. doi: 10.21037/tcr-21-2470. Transl Cancer Res. 2022. PMID: 35571655 Free PMC article.
-
Identification of novel prognostic targets in glioblastoma using bioinformatics analysis.Biomed Eng Online. 2022 Apr 18;21(1):26. doi: 10.1186/s12938-022-00995-8. Biomed Eng Online. 2022. PMID: 35436915 Free PMC article.
-
Characterization of ferroptosis signature to evaluate the predict prognosis and immunotherapy in glioblastoma.Aging (Albany NY). 2021 Jul 9;13(13):17655-17672. doi: 10.18632/aging.203257. Epub 2021 Jul 9. Aging (Albany NY). 2021. PMID: 34244461 Free PMC article.
-
Ferroptosis-Related Gene Contributes to Immunity, Stemness and Predicts Prognosis in Glioblastoma Multiforme.Front Neurol. 2022 Mar 10;13:829926. doi: 10.3389/fneur.2022.829926. eCollection 2022. Front Neurol. 2022. PMID: 35359663 Free PMC article.
-
Identification of ferroptosis genes in immune infiltration and prognosis in thyroid papillary carcinoma using network analysis.BMC Genomics. 2021 Jul 27;22(1):576. doi: 10.1186/s12864-021-07895-6. BMC Genomics. 2021. PMID: 34315405 Free PMC article.
Cited by
-
Network-targeting combination therapy of leptomeningeal glioblastoma using multiple synthetic lethal strategies: a case report.Front Oncol. 2023 Oct 31;13:1210224. doi: 10.3389/fonc.2023.1210224. eCollection 2023. Front Oncol. 2023. PMID: 38023264 Free PMC article.
-
AKR1C1 overexpression leads to lenvatinib resistance in hepatocellular carcinoma.J Gastrointest Oncol. 2023 Jun 30;14(3):1412-1433. doi: 10.21037/jgo-23-277. J Gastrointest Oncol. 2023. PMID: 37435231 Free PMC article.
-
IFNγ regulates ferroptosis in KFs by inhibiting the expression of SPOCD1 through DNMT3A.Cell Death Discov. 2025 Jan 16;11(1):9. doi: 10.1038/s41420-024-02257-z. Cell Death Discov. 2025. PMID: 39820341 Free PMC article.
-
Significance of macrophage infiltration in the prognosis of lung adenocarcinoma patients evaluated by scRNA and bulkRNA analysis.Front Immunol. 2022 Oct 12;13:1028440. doi: 10.3389/fimmu.2022.1028440. eCollection 2022. Front Immunol. 2022. PMID: 36311801 Free PMC article.
-
RNAseq profiling of blood from patients with coronary artery disease: Signature of a T cell imbalance.J Mol Cell Cardiol Plus. 2023 Jun;4:100033. doi: 10.1016/j.jmccpl.2023.100033. Epub 2023 Mar 25. J Mol Cell Cardiol Plus. 2023. PMID: 37303712 Free PMC article.
References
-
- Adolfsson A., Ackerman M., Brownstein N. C. (2019). To Cluster, or Not to Cluster: An Analysis of Clusterability Methods. Pattern Recognit. 88, 13–26. 10.1016/j.patcog.2018.10.026 - DOI
-
- Bayik D., Zhou Y., Park C., Hong C., Vail D., Silver D. J., et al. (2020). Myeloid-Derived Suppressor Cell Subsets Drive Glioblastoma Growth in a Sex-specific Manner. Cancer Discov. 10 (8), 1210–1225. 10.1158/2159-8290.CD-19-1355 - DOI - PMC - PubMed
-
- Binder Z. A., Thorne A. H., Bakas S., Wileyto E. P., Bilello M., Akbari H., et al. (2018). Epidermal Growth Factor Receptor Extracellular Domain Mutations in Glioblastoma Present Opportunities for Clinical Imaging and Therapeutic Development. Cancer Cell 34 (1), 163–177. 10.1016/j.ccell.2018.06.006 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous