

Secondary infections modify the overall course of hospitalized patients with COVID-19: a retrospective study from a network of hospitals across North India
- PMID: 35720143
- PMCID: PMC8863926
- DOI: 10.1016/j.ijregi.2022.02.008
Secondary infections modify the overall course of hospitalized patients with COVID-19: a retrospective study from a network of hospitals across North India
Abstract
Objective: To gain better insight into the extent of secondary bacterial and fungal infections in hospitalized patients in India, and to assess how these alter the course of coronavirus disease 2019 (COVID-19) so that control measures can be suggested.
Methods: In this retrospective, multicentre study, the data of all patients who tested positive for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) on reverse transcriptase polymerase chain reaction (RT-PCR), admitted to hospital between March 2020 and July 2021, were accessed from the electronic health records of a network of 10 hospitals across five states in North India.
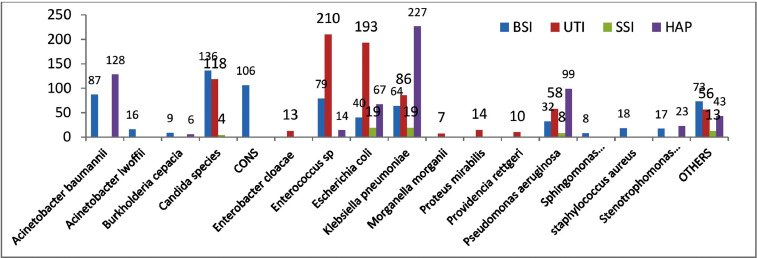
Results: Of 19,852 patients testing positive for SARS-CoV-2 on RT-PCR and admitted to the study hospitals during the study period, 1940 (9.8%) patients developed secondary infections (SIs). Patients with SIs were, on average, 8 years older than patients without SIs (median age 62.6 vs 54.3 years; P<0.001). The risk of SIs was significantly (P<0.001) associated with age, severity of disease at admission, diabetes, admission to the intensive care unit (ICU), and ventilator use. The most common site of infection was urine (41.7%), followed by blood (30.8%) and sputum/bronchoalveolar lavage/endotracheal fluid (24.8%); the least common was pus/wound discharge (2.6%). Gram-negative bacilli (GNB) were the most common organisms (63.2%), followed by Gram-positive cocci (GPC) (19.6%) and fungi (17.3%). Most patients with SIs were on multiple antimicrobials. The most commonly used antibiotics against GNB were beta-lactam/beta-lactamase inhibitors (76.9%), carbapenems (57.7%), cephalosporins (53.9%), and antibiotics against carbapenem-resistant Enterobacteriaceae (47.1%). Empirical use of antibiotics against GPC was seen in 58.9% of patients with SIs, and empirical use of antifungals was observed in 56.9% of patients with SIs. The average length of hospital stay for patients with SIs was almost twice as long as that of patients without SIs (median 13 vs 7 days). Overall mortality among patients with SIs (40.3%) was more than eight times higher than that among patients without SIs (4.6%). Only 1.2% of patients with SIs with mild COVID-19 at admission died, compared with 17.5% of those with moderate COVID-19 at admission and 58.5% of those with severe COVID-19 at admission (P<0.001). The mortality rate was highest in patients with bloodstream infections (49.8%), followed by those with hospital-acquired pneumonia (47.9%), urinary tract infections (29.4%), and skin and soft tissue infections (29.4%). The mortality rate in patients with diabetes with SIs was 45.2%, compared with 34.3% in those without diabetes (P<0.001).
Conclusions: SIs complicate the course of patients hospitalized with COVID-19. These patients tend to have a much longer hospital stay, a higher requirement for oxygen and ICU care, and a significantly higher mortality rate compared with those without SIs. The groups most vulnerable to SIs are patients with more severe COVID-19, elderly patients and patients with diabetes. Judicious empirical use of combination antimicrobials in these groups of vulnerable patients can save lives. It is desirable to have region- or country-specific guidelines for appropriate use of antibiotics and antifungals to prevent their overuse.
Keywords: Antimicrobials; Bacteria; COVID-19; Fungi; Secondary infections.
© 2022 The Author(s).
Figures
Similar articles
-
Safety and Efficacy of Imatinib for Hospitalized Adults with COVID-19: A structured summary of a study protocol for a randomised controlled trial.Trials. 2020 Oct 28;21(1):897. doi: 10.1186/s13063-020-04819-9. Trials. 2020. PMID: 33115543 Free PMC article.
-
Bacterial and fungal co-infections among ICU COVID-19 hospitalized patients in a Palestinian hospital: a retrospective cross-sectional study.F1000Res. 2022 Jan 11;11:30. doi: 10.12688/f1000research.74566.2. eCollection 2022. F1000Res. 2022. PMID: 35811795 Free PMC article.
-
Secondary Infections in Hospitalized COVID-19 Patients: Indian Experience.Infect Drug Resist. 2021 May 24;14:1893-1903. doi: 10.2147/IDR.S299774. eCollection 2021. Infect Drug Resist. 2021. PMID: 34079300 Free PMC article.
-
State-of-the-art review of secondary pulmonary infections in patients with COVID-19 pneumonia.Infection. 2021 Aug;49(4):591-605. doi: 10.1007/s15010-021-01602-z. Epub 2021 Mar 11. Infection. 2021. PMID: 33709380 Free PMC article. Review.
-
Cefiderocol: A Siderophore Cephalosporin with Activity Against Carbapenem-Resistant and Multidrug-Resistant Gram-Negative Bacilli.Drugs. 2019 Feb;79(3):271-289. doi: 10.1007/s40265-019-1055-2. Drugs. 2019. PMID: 30712199 Review.
Cited by
-
Incidence of Bacterial and Fungal Secondary Infections in COVID-19 Patients Admitted to the ICU.Int J Gen Med. 2022 Sep 24;15:7475-7485. doi: 10.2147/IJGM.S382687. eCollection 2022. Int J Gen Med. 2022. PMID: 36187162 Free PMC article.
-
Incidence of secondary bacterial infections and risk factors for in-hospital mortality among coronavirus disease 2019 subjects admitted to secondary care hospital: A single-center cross-sectional retrospective study.Int J Crit Illn Inj Sci. 2024 Apr-Jun;14(2):94-100. doi: 10.4103/ijciis.ijciis_71_23. Epub 2024 Jun 21. Int J Crit Illn Inj Sci. 2024. PMID: 39005973 Free PMC article.
References
-
- Budhiraja S, Indrayan A, Aggarwal M, Jha V, Jain D, Tarai B, et al. Differentials in the characteristics of COVID-19 cases in Wave-1 and Wave-2 admitted to a network of hospitals in North India. medRxiv 2021.06.24.21259438. doi:10.1101/2021.06.24.21259438. https://medrxiv.org/cgi/content/short/2021.06.24.21259438v1. - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous
