

A Phase I Study of Locoregional High-Dose Autologous Natural Killer Cell Therapy With Hepatic Arterial Infusion Chemotherapy in Patients With Locally Advanced Hepatocellular Carcinoma
- PMID: 35720374
- PMCID: PMC9202498
- DOI: 10.3389/fimmu.2022.879452
A Phase I Study of Locoregional High-Dose Autologous Natural Killer Cell Therapy With Hepatic Arterial Infusion Chemotherapy in Patients With Locally Advanced Hepatocellular Carcinoma
Abstract
Background: To explore the feasibility and safety of natural killer (NK) cell therapy in HCC, we performed a prospective, open-label, phase I trial to evaluate the synergistic effect of locoregional high-dose autologous NK cell therapy in combination with hepatic arterial infusion chemotherapy (HAIC).
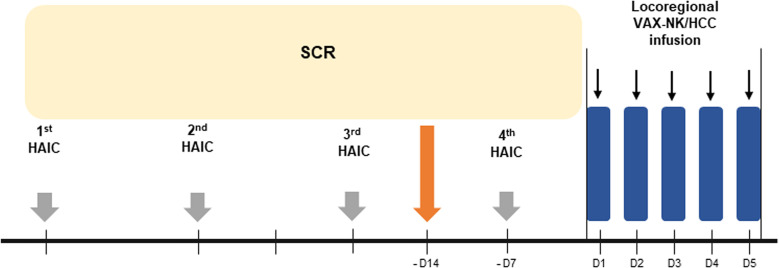
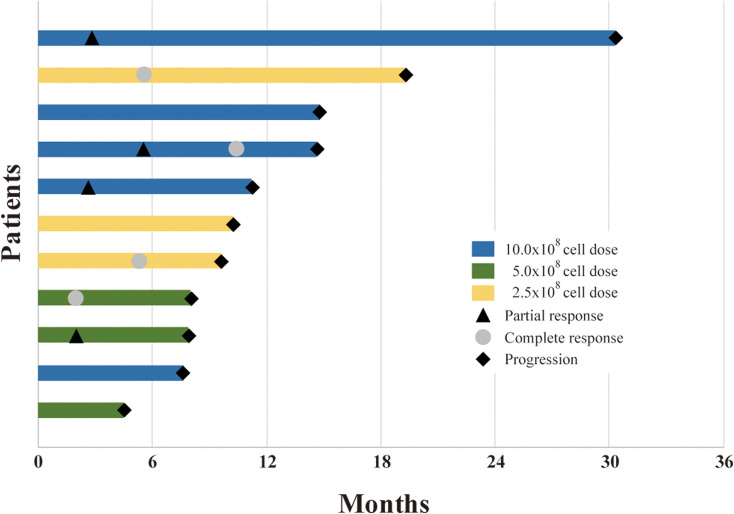
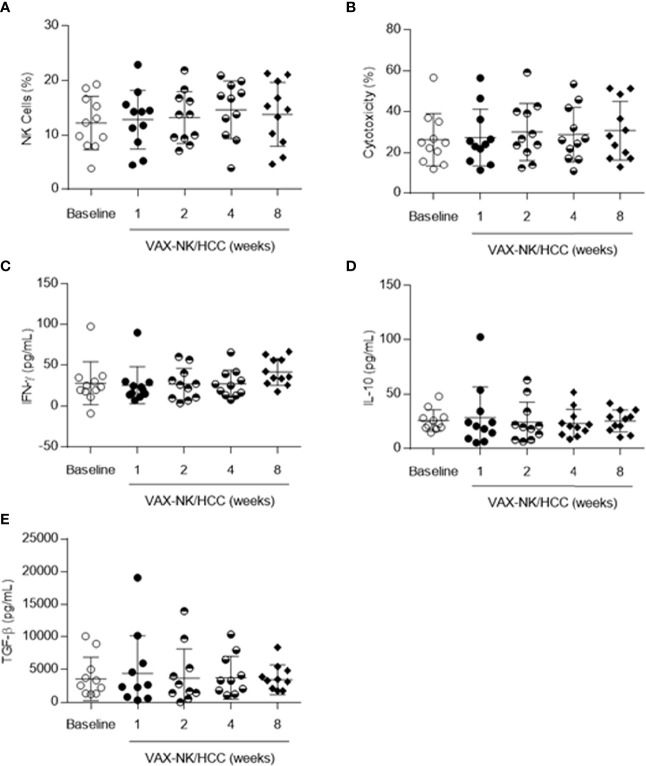
Methods: Patients with locally advanced HCC who were refractory to the standard treatment were eligible for this study. Patients received expanded and activated NK cells for 5 consecutive days in a dose-escalating manner (dose 2.5×108, 5×108, 10×108 NK cells/injection) through hepatic arterial infusion following 4 cycles of HAIC with 5-fluorouracil (750 mg/m2) and cisplatin (25 mg/m2). The primary endpoint was the safety of NK cell-based immunotherapy, and the secondary endpoints were objective response rate (ORR), progression-free survival (PFS), overall survival (OS), and immunologic responses.
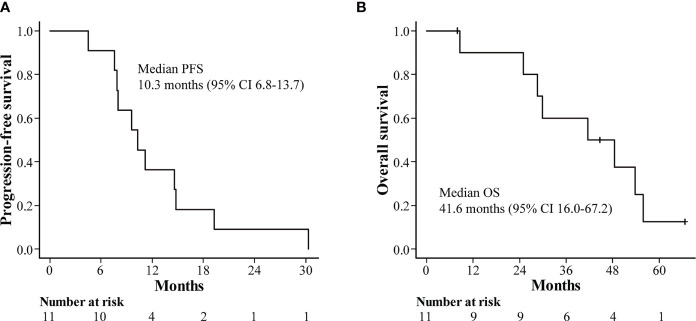
Results: Of the 11 patients enrolled, the confirmed ORR was 63.6% (complete response [CR]: 36.4%, confirmed partial response [PR]: 27.3%). Stable disease (SD) and progressive disease (PD) were observed in two patients (18.2%) each, resulting in a disease control rate (DCR) of 81.8%. The median PFS and OS were 10.3 and 41.6 months, respectively. There were no incidences of decompensation or severe adverse events during HAIC, and no adverse events related to NK cell infusion were noted.
Conclusion: The combination of HAIC and locoregional high-dose NK cell therapy is a safe and effective treatment for locally advanced HCC patients who were refractory to the standard treatment. This result warrants further development of this novel treatment to establish its efficacy in HCC.
Clinical trial registration: cris.nih.go.kr, identifier KCT0003973.
Keywords: autologous; clinical trial; hepatic arterial infusion chemotherapy (HAIC); hepatocellular carcinoma; natural killer (NK) cell.
Copyright © 2022 Bae, Lee, Kim, Lee, Chung, Cho and Koh.
Conflict of interest statement
JL is employed by Vaxcell-Bio Therapeutics. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials