

Chest Pain Network with Support of Telemedicine: Impact on Reperfusion Therapy and Clinical Outcomes After 8 Years of Experience
- PMID: 35720760
- PMCID: PMC8812289
- DOI: 10.1089/tmr.2021.0033
Chest Pain Network with Support of Telemedicine: Impact on Reperfusion Therapy and Clinical Outcomes After 8 Years of Experience
Abstract
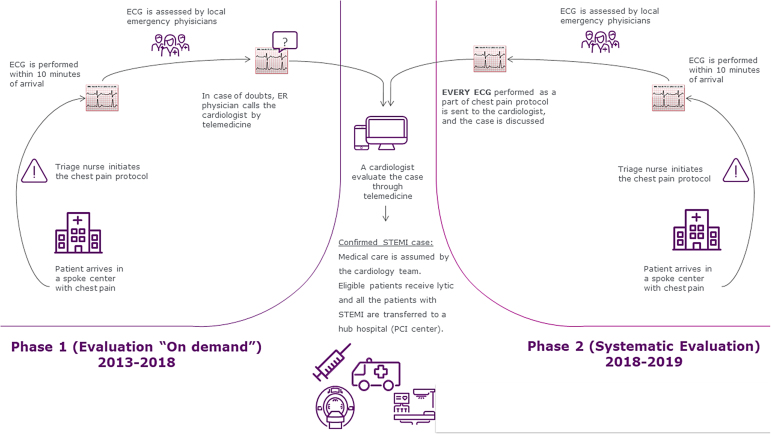
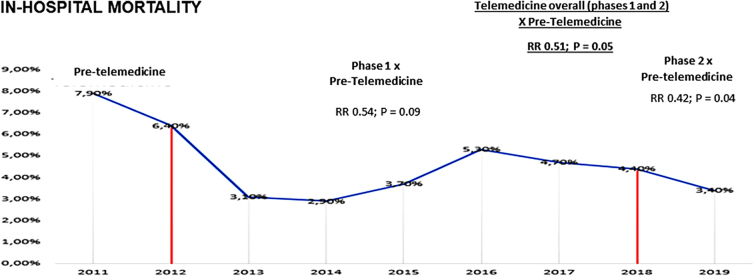
Background: Different approaches of evaluation by cardiologists using telemedicine have the potential of improving care of patients with ST elevation myocardial infarction (STEMI). Objective: To compare the use of pharmacoinvasive strategy and associated clinical outcomes (heart failure [HF] and mortality) among patients with STEMI before and after a program of telemedicine and also according to the level of support by telemedicine. Methods: A chest pain network with the support of a cardiologist through telemedicine was implemented in 2012 in 22 emergency departments without a local cardiac catheterization laboratory. Initially (phase 1 of telemedicine), the decision to discuss the case with the cardiologist was based on the judgment of the emergency physician. At the end of 2018, the use of telemedicine was modified and a dedicated cardiologist was available continuously to discuss systematically all suspected cases (phase 2 of telemedicine). The use of fibrinolytics and the rates of HF and in-hospital mortality were compared among three different periods: pretelemedicine (2011), and phase 1 and phase 2 of the telemedicine program. Results: We evaluated 1034 STEMI patients and after comparing the three phases, we did not find significant differences regarding age, gender, and comorbidities. The use of fibrinolytics before transferring STEMI patients to a percutaneous coronary intervention center (pharmacoinvasive strategy) increased after telemedicine implementation (38% vs. 65.2%; p < 0.01), which was associated with a lower rate of HF (23.9% vs. 14.4%; p = 0.01) and death (7.9% vs. 4.0%; p = 0.05). The in-hospital mortality was lower in phase 2 with systematic evaluation by telemedicine compared with pretelemedicine (7.9% vs. 3.3%; p = 0.04). Conclusion: The implementation of a systematic and organized chest pain protocol, including telemedicine support, was associated with a significant increase in the use of pharmacoinvasive strategy and better clinical patient outcomes in patients with STEMI. Our findings provide important insights on how to improve the management of this high-risk population, reducing the gap between evidence and clinical practice.
Keywords: ST-segment elevation myocardial infarction; acute coronary syndrome; telemedicine.
© United Health Group Brazil, 2021; Published by Mary Ann Liebert, Inc.
Conflict of interest statement
P.G.M.B.S. reports grants and personal fees from Pfizer, Bayer, and Roche Diagnostics outside the submitted work. R.D.L. reports grants from Amgen; personal fees from Bayer, Boehringer Ingelheim, and Portola; and grants and personal fees from Bristol Myers Squibb, Glaxo Smith Kline, Pfizer, and Sanofi-Aventis outside the submitted work. All other authors have no disclosures to report.
Figures
Similar articles
-
Impact of Chest Pain Protocol with Access to Telemedicine on Implementation of Pharmacoinvasive Strategy in a Private Hospital Network.Telemed J E Health. 2016 Jul;22(7):549-52. doi: 10.1089/tmj.2015.0178. Epub 2015 Dec 22. Telemed J E Health. 2016. PMID: 26693879
-
Pharmacoinvasive Strategy Versus Primary Percutaneous Coronary Intervention in ST-Elevation Myocardial Infarction in Clinical Practice: Insights From the Vital Heart Response Registry.Circ Cardiovasc Interv. 2019 Oct;12(10):e008059. doi: 10.1161/CIRCINTERVENTIONS.119.008059. Epub 2019 Oct 14. Circ Cardiovasc Interv. 2019. PMID: 31607152
-
Efficacy and Safety of Pharmacoinvasive Strategy Compared to Primary Percutaneous Coronary Intervention in the Management of ST-Segment Elevation Myocardial Infarction: A Prospective Country-Wide Registry.Ann Glob Health. 2020 Feb 5;86(1):13. doi: 10.5334/aogh.2632. Ann Glob Health. 2020. PMID: 32064231 Free PMC article.
-
Emergency percutaneous coronary intervention (PCI) for the care of patients with ST-elevation myocardial infarction (STEMI).Minerva Cardioangiol. 2007 Oct;55(5):593-623. Minerva Cardioangiol. 2007. PMID: 17912165 Review.
-
Management of prehospital thrombolytic therapy in ST-segment elevation acute coronary syndrome (<12 hours).Minerva Anestesiol. 2005 Jun;71(6):297-302. Minerva Anestesiol. 2005. PMID: 15886591 Review.
Cited by
-
Impact of COVID-19 on door-to-wire time in ST-segment elevation myocardial infarction treatment: the role of digital communication.BMC Cardiovasc Disord. 2025 Mar 12;25(1):173. doi: 10.1186/s12872-025-04618-7. BMC Cardiovasc Disord. 2025. PMID: 40075270 Free PMC article.
References
-
- Cenko E, Ricci B, Kedev S, et al. . Reperfusion therapy for ST-elevation acute myocardial infarction in Eastern Europe: the ISACS-TC registry. Eur Heart J Qual Care Clin Outcomes 2016;2:45–51. - PubMed
-
- Peterson ED, Roe MT, Mulgund J, et al. . Association between hospital process performance and outcomes among patients with acute coronary syndromes. JAMA 2006;295:1912–1920. - PubMed
-
- Longenecker JC, Alfaddagh A, Zubaid M, et al. . Adherence to ACC/AHA performance measures for myocardial infarction in six Middle-Eastern countries: association with in-hospital mortality and clinical characteristics. Int J Cardiol 2013;167:1406–1411. - PubMed
-
- Barbagelata A, Perna ER, Clemmensen P, et al. . Time to reperfusion in acute myocardial infarction. It is time to reduce it!. J Electrocardiol 2007;40:257–264. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous