

Management of hepatorenal syndrome in liver cirrhosis: a recent update
- PMID: 35721838
- PMCID: PMC9201357
- DOI: 10.1177/17562848221102679
Management of hepatorenal syndrome in liver cirrhosis: a recent update
Abstract
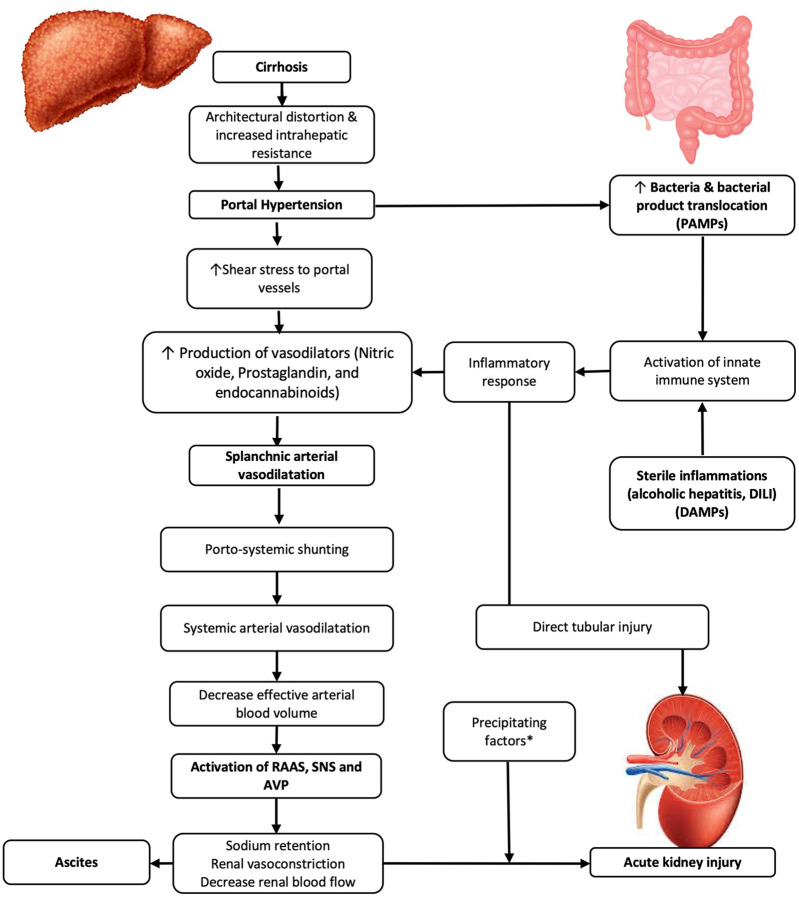
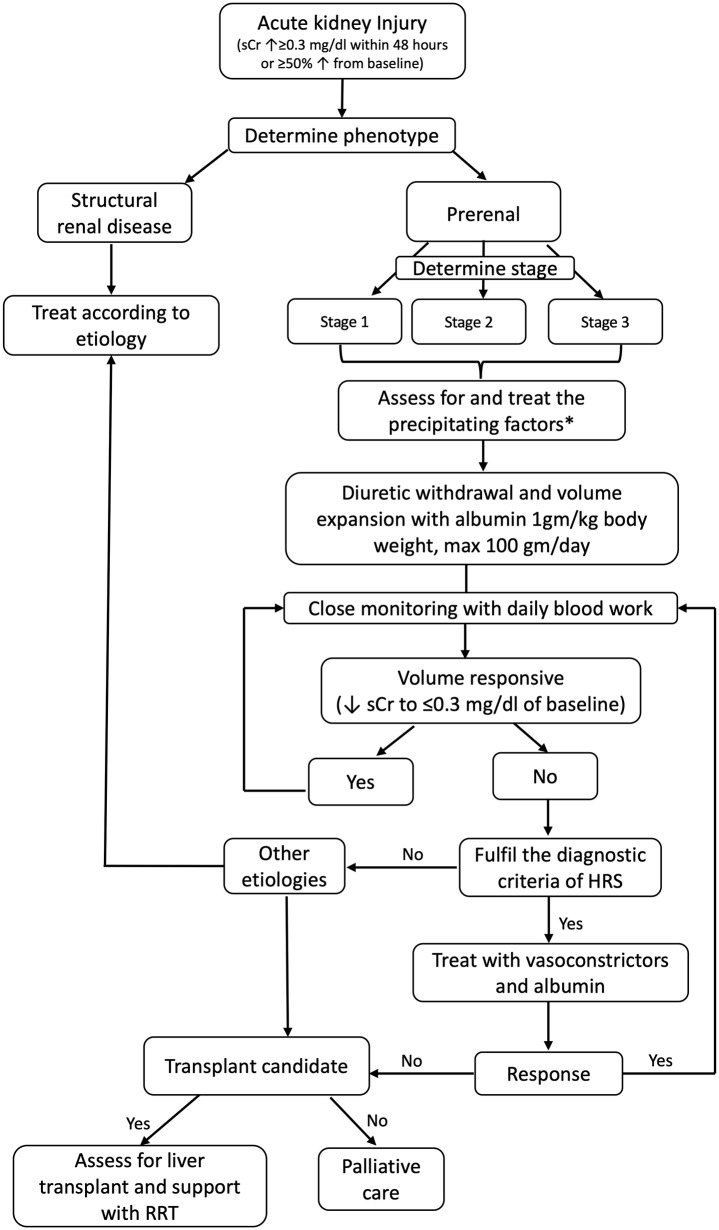
Hepatorenal syndrome (HRS) is a serious form of renal dysfunction in patients with cirrhosis and ascites. It is an important component of the acute-on-chronic liver failure (ACLF) syndrome. Significant recent changes in the understanding of the pathophysiology of renal dysfunction in cirrhosis include the role of inflammation in addition to hemodynamic changes. The term acute kidney injury (AKI) is now adopted to include all functional and structural forms of acute renal dysfunction in cirrhosis, with various stages describing the severity of the condition. Type 1 hepatorenal syndrome (HRS1) is renamed HRS-AKI, which is stage 2 AKI [doubling of baseline serum creatinine (sCr)] while fulfilling all other criteria of HRS1. Albumin is used for its volume expanding and anti-inflammatory properties to confirm the diagnosis of HRS-AKI. Vasoconstrictors are added to albumin as pharmacotherapy to improve the hemodynamics. Terlipressin, although not yet available in North America, is the most common vasoconstrictor used worldwide. Patients with high grade of ACLF treated with terlipressin are at risk for respiratory failure if there is pretreatment respiratory compromise. Norepinephrine is equally effective as terlipressin in reversing HRS1. Recent data show that norepinephrine may be administered outside the intensive care setting, but close monitoring is still required. There has been no improvement in overall or transplant-free survival shown with vasoconstrictor use, but response to vasoconstrictors with reduction in sCr is associated with improvement in survival. Non-responders to vasoconstrictor plus albumin will need liver transplantation as definite treatment with renal replacement therapy as a bridge therapy. Combined liver and kidney transplantation is recommended for patients with prolonged history of AKI, underlying chronic kidney disease or with hereditary renal conditions. Future developments, such as the use of biomarkers and metabolomics, may help to identify at risk patients with earlier diagnosis to allow for earlier treatment with improved outcomes.
Keywords: HRS-AKI; inflammation; liver transplantation; terlipressin; vasoconstrictors.
© The Author(s), 2022.
Conflict of interest statement
Conflict of interest statement: Mallinckrodt Pharmaceutical: Consultant and research grant provided to the institution.
Figures
References
-
- Tsien CD, Rabie R, Wong F. Acute kidney injury in decompensated cirrhosis. Gut 2013; 62: 131–137. - PubMed
-
- de Carvalho JR, Villela-Nogueira CA, Luiz RR, et al.. Acute kidney injury network criteria as a predictor of hospital mortality in cirrhotic patients with ascites. J Clin Gastroenterol 2012; 46: e21–e26. - PubMed
-
- Arroyo V, Gines P, Gerbes AL, et al.. Definition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis. International Ascites Club. Hepatology 1996; 23: 164–176. - PubMed
-
- Wong F, Nadim MK, Kellum JA, et al.. Working Party proposal for a revised classification system of renal dysfunction in patients with cirrhosis. Gut 2011; 60: 702–709. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
