

Clinical Outcomes Following Hemodynamic Parameter or Intravascular Imaging-Guided Percutaneous Coronary Intervention in the Era of Drug-Eluting Stents: An Updated Systematic Review and Bayesian Network Meta-Analysis of 28 Randomized Trials and 11,860 Patients
- PMID: 35722113
- PMCID: PMC9203695
- DOI: 10.3389/fcvm.2022.860189
Clinical Outcomes Following Hemodynamic Parameter or Intravascular Imaging-Guided Percutaneous Coronary Intervention in the Era of Drug-Eluting Stents: An Updated Systematic Review and Bayesian Network Meta-Analysis of 28 Randomized Trials and 11,860 Patients
Abstract
Background: Coronary angiography (CAG) is the standard imaging modality for guiding percutaneous coronary interventions (PCI). Intracoronary imaging techniques such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), and hemodynamic parameter like fractional flow reserve (FFR) can overcome some limitations of CAG.
Objective: We sought to explore the clinical outcomes of different PCI guidance modalities in the era of drug-eluting stent (DES).
Methods: A network meta-analysis of 28 randomized trials and 11,860 patients undergoing different modalities-guided PCI in the era of DES was performed. Odds ratio (OR) with 95% credible interval (CrI) were calculated.
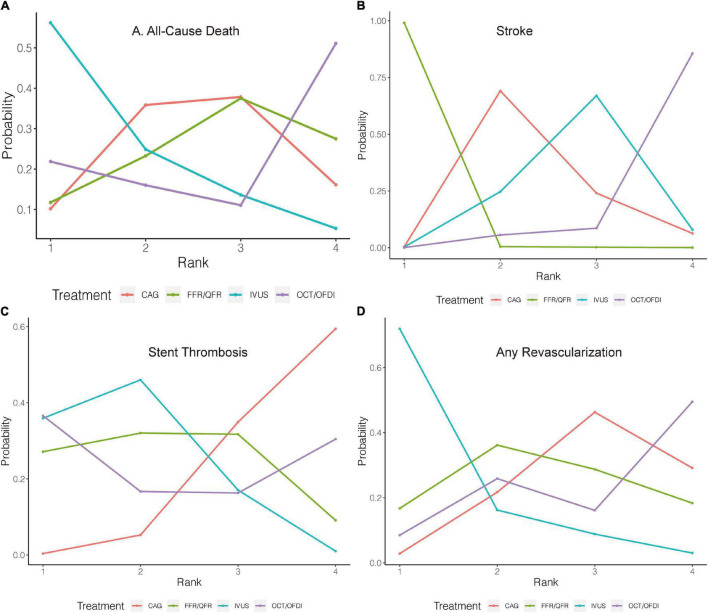
Results: In comparison with CAG, IVUS was associated with a significant reduction in major adverse cardiovascular events (MACE, OR: 0.60; 95% CrI: 0.46-0.79), cardiovascular death (OR: 0.46; 95% CrI: 0.20-0.94), target vessel/lesion revascularization (TVR/TLR, OR: 0.55; 95% CrI: 0.41-0.74), and a trend toward decreased risk of stent thrombosis (OR: 0.44; 95% CrI: 0.17 to 1.00). FFR/quantitative flow ratio (QFR) could significantly reduce stroke compared with CAG, IVUS, and OCT/optical frequency domain imaging (OFDI). However, myocardial infarction (MI), all-cause death, stent thrombosis, and any revascularization presented similar risks for different PCI guidance modalities.
Conclusion: In the era of DES, IVUS led to lower risks of MACE than CAG, which was mainly due to lower risks of cardiovascular death and TVR/TLR. A trend toward decreased risk of stent thrombosis was also observed with IVUS. Hemodynamic parameter (FFR/QFR)-guided PCI could significantly reduce the stroke risk compared with CAG, IVUS, and OCT/OFDI.
Systematic review registration: [https://www.crd.york.ac.uk/PROSPERO/], identifier [CRD42021291442].
Keywords: coronary angiography; drug-eluting stent (DES); fractional flow reserve (FFR); intravascular ultrasound (IVUS); optical coherence tomography (OCT); percutaneous coronary interventions (MeSH: D062645).
Copyright © 2022 Hu, Tan, Yin, Zhao, Gao, Yang and Yang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Tian NL, Gami SK, Ye F, Zhang JJ, Liu ZZ, Lin S, et al. Angiographic and clinical comparisons of intravascular ultrasound- versus angiography-guided drug-eluting stent implantation for patients with chronic total occlusion lesions: two-year results from a randomised AIR-CTO study. EuroIntervention. (2015) 10:1409–17. 10.4244/EIJV10I12A245 - DOI - PubMed
-
- Zhang J, Gao X, Kan J, Ge Z, Han L, Lu S, et al. Intravascular ultrasound versus angiography-guided drug-eluting stent implantation: the ULTIMATE trial. J Am Coll Cardiol. (2018) 72:3126–37. - PubMed
-
- Onuma Y, Kogame N, Sotomi Y, Miyazaki Y, Asano T, Takahashi K, et al. A randomized trial evaluating online 3-dimensional optical frequency domain imaging-guided percutaneous coronary intervention in bifurcation lesions. Circ Cardiovasc Interv. (2020) 13:e009183. 10.1161/CIRCINTERVENTIONS.120.009183 - DOI - PMC - PubMed
-
- Layland J, Oldroyd KG, Curzen N, Sood A, Balachandran K, Das R, et al. Fractional flow reserve vs. angiography in guiding management to optimize outcomes in non-ST-segment elevation myocardial infarction: the British heart foundation FAMOUS-NSTEMI randomized trial. Eur Heart J. (2015) 36:100–11. 10.1093/eurheartj/ehu338 - DOI - PMC - PubMed
-
- Park SH, Jeon KH, Lee JM, Nam CW, Doh JH, Lee BK, et al. Long-term clinical outcomes of fractional flow reserve-guided versus routine drug-eluting stent implantation in patients with intermediate coronary stenosis: five-year clinical outcomes of DEFER-DES trial. Circ Cardiovasc Interv. (2015) 8:e002442. 10.1161/CIRCINTERVENTIONS.115.002442 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous