

Acute multifocal retinitis in a patient with Q fever (Coxiella Burnetii infection) with endocarditis
- PMID: 35723746
- PMCID: PMC9209575
- DOI: 10.1186/s12348-022-00295-1
Acute multifocal retinitis in a patient with Q fever (Coxiella Burnetii infection) with endocarditis
Abstract
Objective: To report acute multifocal retinitis in association with serologically-proven Coxiella (C) Burnetii infection (Q fever) with endocarditis.
Material and methods: A single case report documented with multimodal imaging.
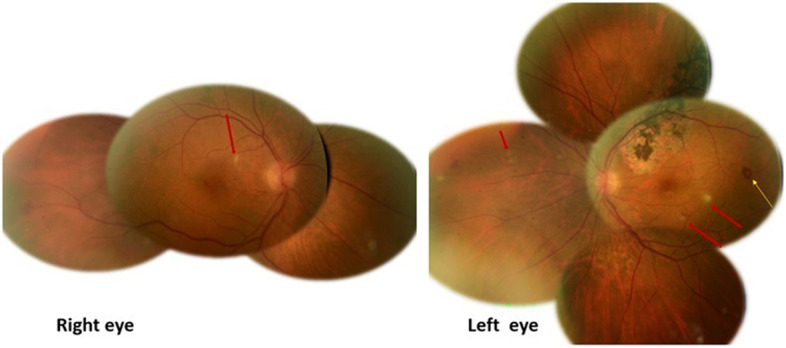
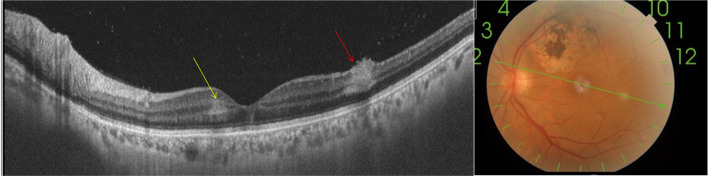
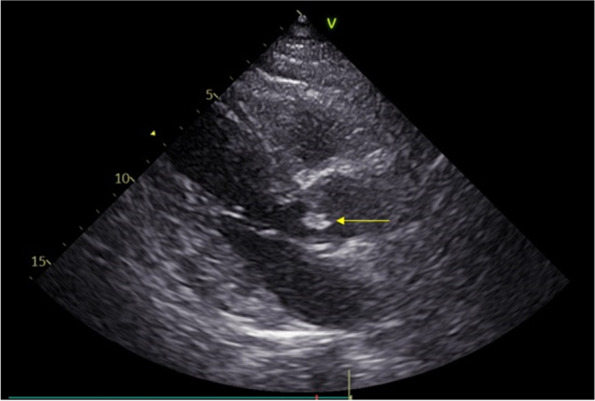
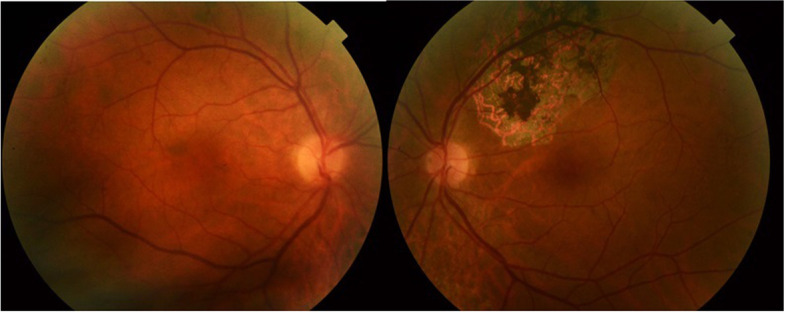
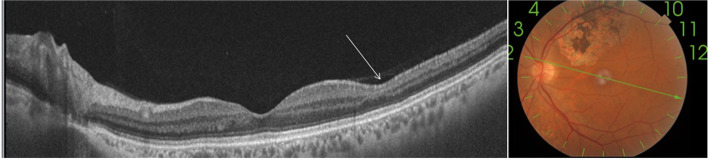
Results: A 67-year-old cattle breeder presented with a 2-week history of persistent fever, headache, and floaters in both eyes. On examination, his best-corrected visual acuity was 20/20, and there was 1+ vitreous cells in both eyes. Bilateral fundus examination showed multiple small superficial white retinal lesions scattered in the posterior pole and midperiphery associated with a few retinal hemorrhages. These retinal lesions did not stain on fluorescein angiography (FA) and showed focal hyperreflectivity and thickening primarily involving the inner retinal layers on optical coherence tomography (OCT). There also was a band-like hyper-reflective area in the middle retina consistent with paramacular acute middle maculopathy. Transthoracic echocardiogram (TTE) showed a mobile echodensity on the anterior aortic leaflet consistent with a diagnosis of endocarditis. Elisa assays performed on paired serum samples collected 2 weeks apart showed increase in antibodies against C burnetii from 60 IU/ml to 255 IU/ml. The patient was treated with doxycycline 100 mg twice a day for 18 months, with subsequent resolution of the endocarditis. Sequential ocular examinations showed gradual resolution of all acute retinal findings without visible scars.
Conclusion: Acute Q fever, caused by C burnetii infection, should be considered in the differential diagnosis of acute multifocal retinitis. A systematic cardiac assessment with echocardiography is essential for early diagnosis of associated endocarditis and for prompt administration of appropriate antibiotic treatment to improve clinical outcomes.
Keywords: Acute Q fever; Acute multifocal retinitis; Coxiella burnetii; endocarditis.
© 2022. The Author(s).
Conflict of interest statement
None of the authors has any financial/conflicting interests to disclose
Figures
Similar articles
-
Q Fever Endocarditis with Bilateral Multifocal Retinitis: A Case Report.J Curr Ophthalmol. 2024 Aug 10;35(4):405-407. doi: 10.4103/joco.joco_81_23. eCollection 2023 Oct-Dec. J Curr Ophthalmol. 2024. PMID: 39281405 Free PMC article.
-
Asymptomatic bilateral acute multifocal retinitis in Q fever endocarditis.BMJ Case Rep. 2025 Jul 16;18(7):e265412. doi: 10.1136/bcr-2025-265412. BMJ Case Rep. 2025. PMID: 40669876
-
Acute Q Fever Endocarditis: A Paradigm Shift Following the Systematic Use of Transthoracic Echocardiography During Acute Q Fever.Clin Infect Dis. 2019 Nov 13;69(11):1987-1995. doi: 10.1093/cid/ciz120. Clin Infect Dis. 2019. PMID: 30785186
-
A contemporary 16-year review of Coxiella burnetii infective endocarditis in a tertiary cardiac center in Queensland, Australia.Infect Dis (Lond). 2018 Jul;50(7):531-538. doi: 10.1080/23744235.2018.1445279. Epub 2018 Mar 8. Infect Dis (Lond). 2018. PMID: 29516748 Review.
-
New insights in Coxiella burnetii infection: diagnosis and therapeutic update.Expert Rev Anti Infect Ther. 2020 Jan;18(1):75-86. doi: 10.1080/14787210.2020.1699055. Epub 2019 Dec 6. Expert Rev Anti Infect Ther. 2020. PMID: 31782315 Review.
Cited by
-
Human-biting ticks and zoonotic tick-borne pathogens in North Africa: diversity, distribution, and trans-Mediterranean public health challenges.One Health. 2023 Apr 22;16:100547. doi: 10.1016/j.onehlt.2023.100547. eCollection 2023 Jun. One Health. 2023. PMID: 37363219 Free PMC article. Review.
-
Q Fever Endocarditis with Bilateral Multifocal Retinitis: A Case Report.J Curr Ophthalmol. 2024 Aug 10;35(4):405-407. doi: 10.4103/joco.joco_81_23. eCollection 2023 Oct-Dec. J Curr Ophthalmol. 2024. PMID: 39281405 Free PMC article.
-
Clinical features of infectious uveitis in a Tunisian population.Tunis Med. 2023 Feb 11;101(2):259-265. Tunis Med. 2023. PMID: 37682270 Free PMC article. English.
-
Ophthalmic implications of biological threat agents according to the chemical, biological, radiological, nuclear, and explosives framework.Front Med (Lausanne). 2024 Jan 16;10:1349571. doi: 10.3389/fmed.2023.1349571. eCollection 2023. Front Med (Lausanne). 2024. PMID: 38293299 Free PMC article. Review.
-
Epidemiological spectrum of infectious uveitis in the Asia-Pacific.Taiwan J Ophthalmol. 2025 Jun 10;15(2):157-181. doi: 10.4103/tjo.TJO-D-25-00052. eCollection 2025 Apr-Jun. Taiwan J Ophthalmol. 2025. PMID: 40584206 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
