

Gut Factors Mediating the Physiological Impact of Bariatric Surgery
- PMID: 35723770
- PMCID: PMC12077241
- DOI: 10.1007/s11892-022-01478-9
Gut Factors Mediating the Physiological Impact of Bariatric Surgery
Abstract
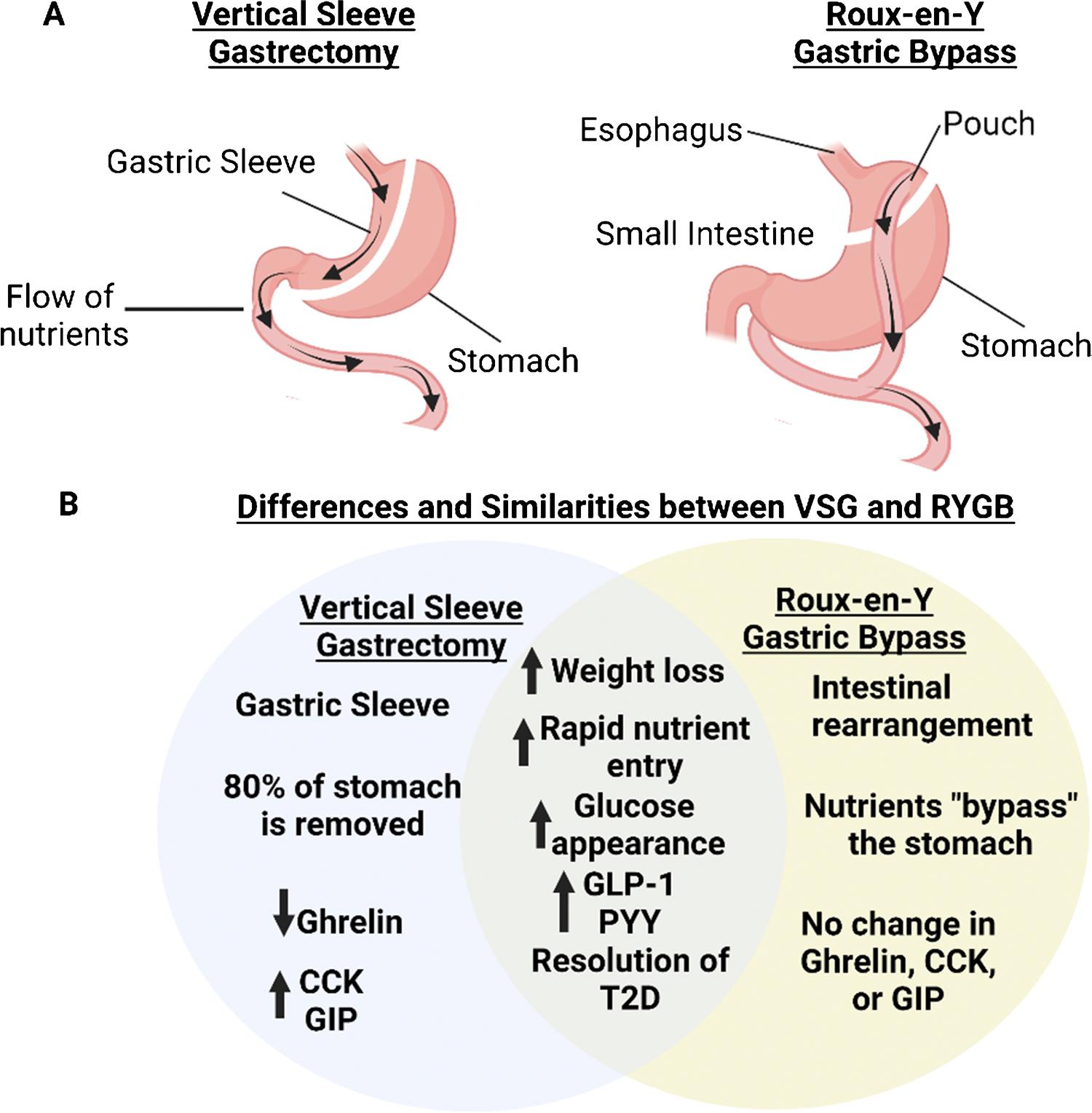
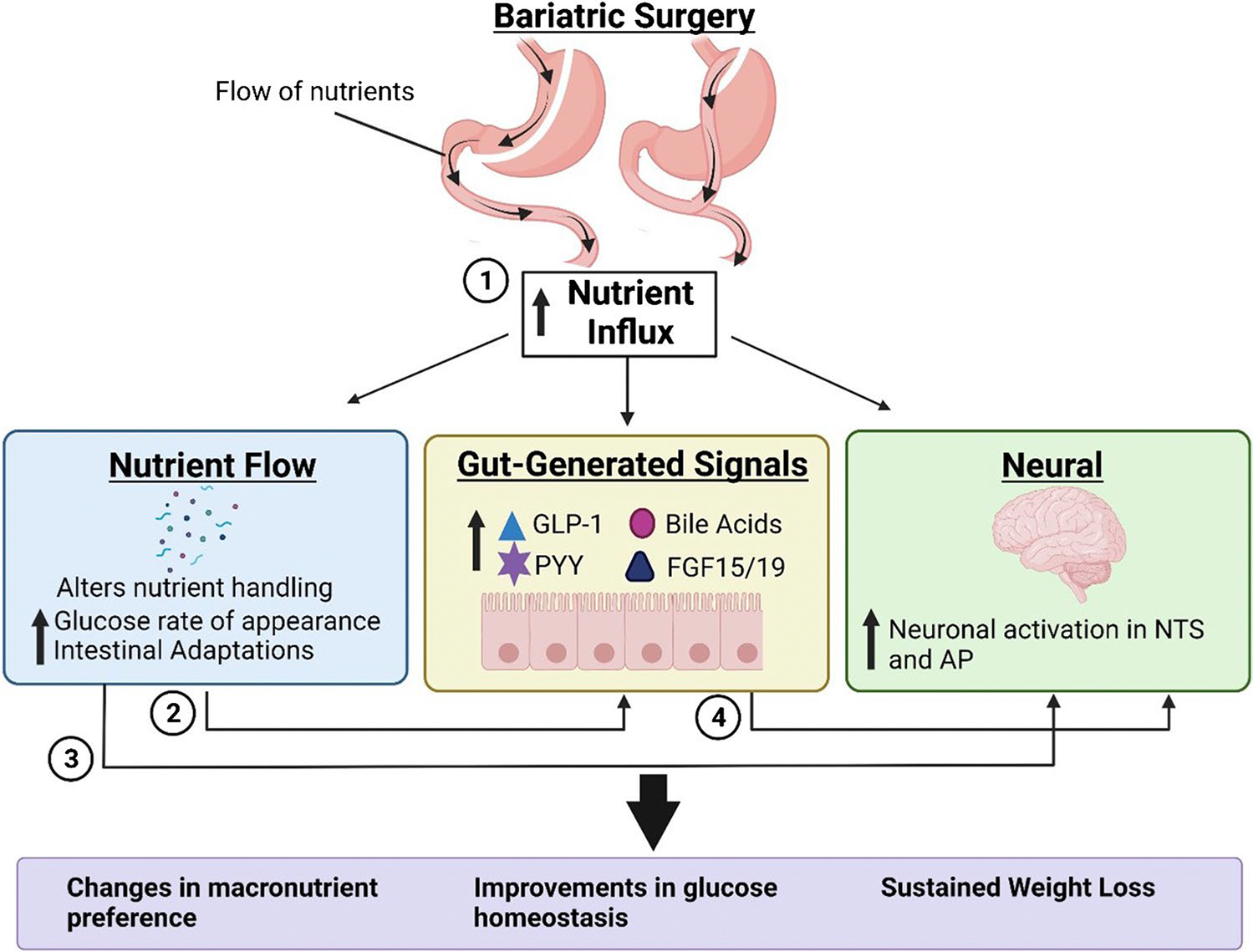
Despite decades of obesity research and various public health initiatives, obesity remains a major public health concern. Our most drastic but most effective treatment of obesity is bariatric surgery with weight loss and improvements in co-morbidities, including resolution of type 2 diabetes (T2D). However, the mechanisms by which surgery elicits metabolic benefits are still not well understood. One proposed mechanism is through signals generated by the intestine (nutrients, neuronal, and/or endocrine) that communicate nutrient status to the brain. In this review, we discuss the contributions of gut-brain communication to the physiological regulation of body weight and its impact on the success of bariatric surgery. Advancing our understanding of the mechanisms that drive bariatric surgery-induced metabolic benefits will ultimately lead to the identification of novel, less invasive strategies to treat obesity.
Keywords: Bariatric surgery; Gut hormones; Obesity.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Figures
Similar articles
-
Mechanisms facilitating weight loss and resolution of type 2 diabetes following bariatric surgery.Trends Endocrinol Metab. 2010 Jun;21(6):337-44. doi: 10.1016/j.tem.2010.01.006. Epub 2010 Feb 3. Trends Endocrinol Metab. 2010. PMID: 20133150 Review.
-
Molecular insights from bariatric surgery.Rev Endocr Metab Disord. 2011 Sep;12(3):211-7. doi: 10.1007/s11154-011-9172-6. Rev Endocr Metab Disord. 2011. PMID: 21331643 Free PMC article. Review.
-
Potential mechanisms by which bariatric surgery improves systemic metabolism.Transl Res. 2013 Feb;161(2):63-72. doi: 10.1016/j.trsl.2012.09.004. Epub 2012 Oct 16. Transl Res. 2013. PMID: 23079469 Review.
-
Weight Loss and the Prevention and Treatment of Type 2 Diabetes Using Lifestyle Therapy, Pharmacotherapy, and Bariatric Surgery: Mechanisms of Action.Curr Obes Rep. 2015 Jun;4(2):287-302. doi: 10.1007/s13679-015-0155-x. Curr Obes Rep. 2015. PMID: 26627223 Review.
-
Role of gut microbiota, bile acids and their cross-talk in the effects of bariatric surgery on obesity and type 2 diabetes.J Diabetes Investig. 2018 Jan;9(1):13-20. doi: 10.1111/jdi.12687. Epub 2017 Jun 12. J Diabetes Investig. 2018. PMID: 28434196 Free PMC article. Review.
Cited by
-
Obesity- and diet-induced plasticity in systems that control eating and energy balance.Obesity (Silver Spring). 2024 Aug;32(8):1425-1440. doi: 10.1002/oby.24060. Epub 2024 Jul 15. Obesity (Silver Spring). 2024. PMID: 39010249 Free PMC article. Review.
-
Glucose metabolism after bariatric surgery: implications for T2DM remission and hypoglycaemia.Nat Rev Endocrinol. 2023 Mar;19(3):164-176. doi: 10.1038/s41574-022-00757-5. Epub 2022 Oct 26. Nat Rev Endocrinol. 2023. PMID: 36289368 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
