

Pulmonary artery acceleration time accuracy for systolic pulmonary artery pressure estimation in critically ill patients
- PMID: 35723841
- PMCID: PMC9209611
- DOI: 10.1186/s13089-022-00276-4
Pulmonary artery acceleration time accuracy for systolic pulmonary artery pressure estimation in critically ill patients
Abstract
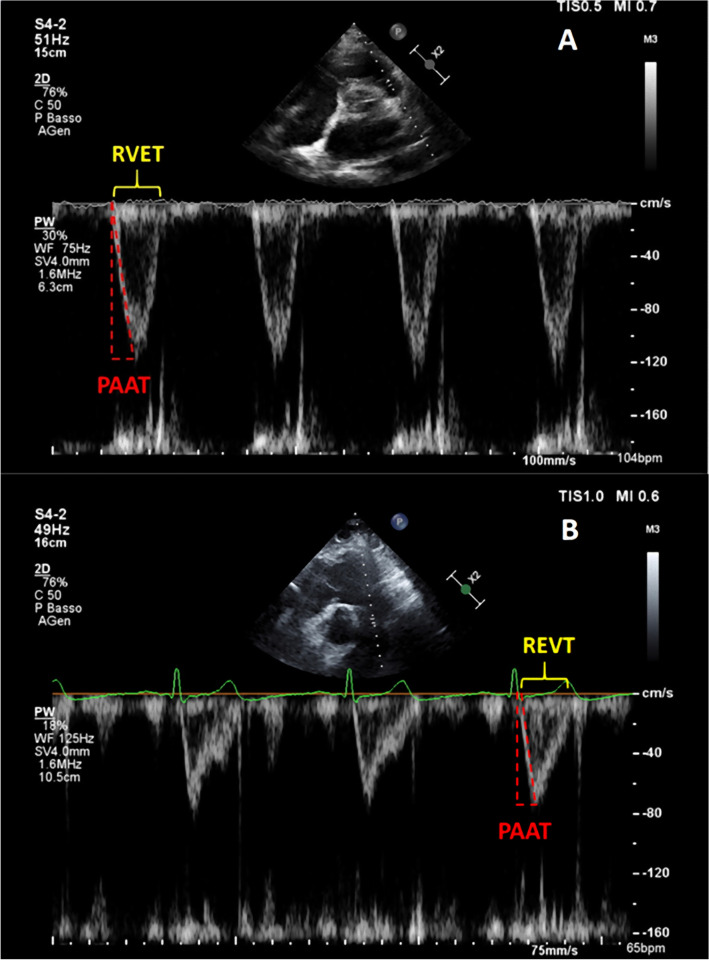
Background: Estimation of pulmonary pressures is of key importance in acute cardiovascular and respiratory failure. Pulmonary artery acceleration time (PAAT) has emerged as reliable parameter for the estimation of systolic pulmonary artery pressure (sPAP) in cardiological population with preserved right ventricular function. We sought to find whether PAAT correlates with sPAP in critically ill patients with and without right ventricular (RV) systolic dysfunction.
Methods: Observational study. We measured sPAP using continuous-wave Doppler analysis of tricuspid regurgitation velocity peak method and we assessed the validity of PAAT in estimating sPAP in patients admitted to adult intensive care unit (ICU) for acute cardiovascular and respiratory failure.
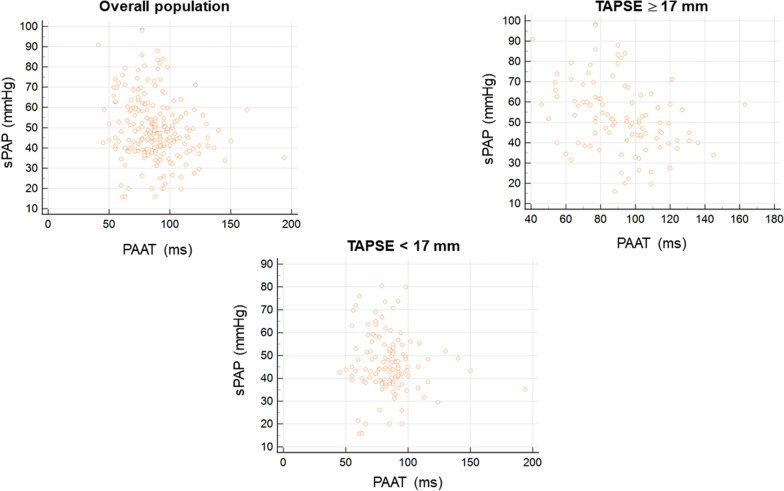
Results: We enrolled 236 patients admitted to cardiothoracic ICU for cardiovascular and respiratory failure (respectively: 129, 54.7% and 107, 45.3%). 114 (48.3%) had preserved RV systolic function (defined as TAPSE ≥ 17 mm), whilst 122 (51.7%) had RV systolic impairment (defined as TAPSE < 17 mm). A weak inverse correlation between PAAT and sPAP (ρ-0.189, p 0.0035) was observed in overall population, which was confirmed in those with preserved RV systolic PAAT and sPAP (ρ-0.361, p 0.0001). In patients with impaired RV systolic function no statistically significant correlation between PAAT and sPAP was demonstrated (p 0.2737). Adjusting PAAT values for log10, heart rate and RV ejection time did not modify the abovementioned correlations.
Conclusions: PAAT measurement to derive sPAP is not reliable in cardiothoracic critically ill patients, particularly in the coexistence of RV systolic impairment.
Keywords: Acute cardiovascular failure; Acute respiratory failure; Pulmonary artery acceleration time; Pulmonary artery pressure; Right ventricular dysfunction.
© 2022. The Author(s).
Conflict of interest statement
FM received fees for lectures from GE Healthcare, Hamilton Medical, SEDA SpA, outside the present work. GT received fees for lectures from GE Healthcare, outside the present work.
Figures
References
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M, Group ESCSD 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Heart J. 2016;37(1):67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
-
- Hellenkamp K, Unsöld B, Mushemi-Blake S, Shah AM, Friede T, Hasenfuß G, Seidler T. Echocardiographic estimation of mean pulmonary artery pressure: a comparison of different approaches to assign the likelihood of pulmonary hypertension. J Am Soc Echocardiogr. 2018;31(1):89–98. doi: 10.1016/j.echo.2017.09.009. - DOI - PubMed
-
- Amsallem M, Sternbach JM, Adigopula S, Kobayashi Y, Vu TA, Zamanian R, Liang D, Dhillon G, Schnittger I, McConnell MV, Haddad F. Addressing the controversy of estimating pulmonary arterial pressure by echocardiography. J Am Soc Echocardiogr. 2016;29(2):93–102. doi: 10.1016/j.echo.2015.11.001. - DOI - PubMed
LinkOut - more resources
Full Text Sources