

Short-term outcome for high-risk patients after esophagectomy
- PMID: 35724560
- PMCID: PMC9817823
- DOI: 10.1093/dote/doac028
Short-term outcome for high-risk patients after esophagectomy
Abstract
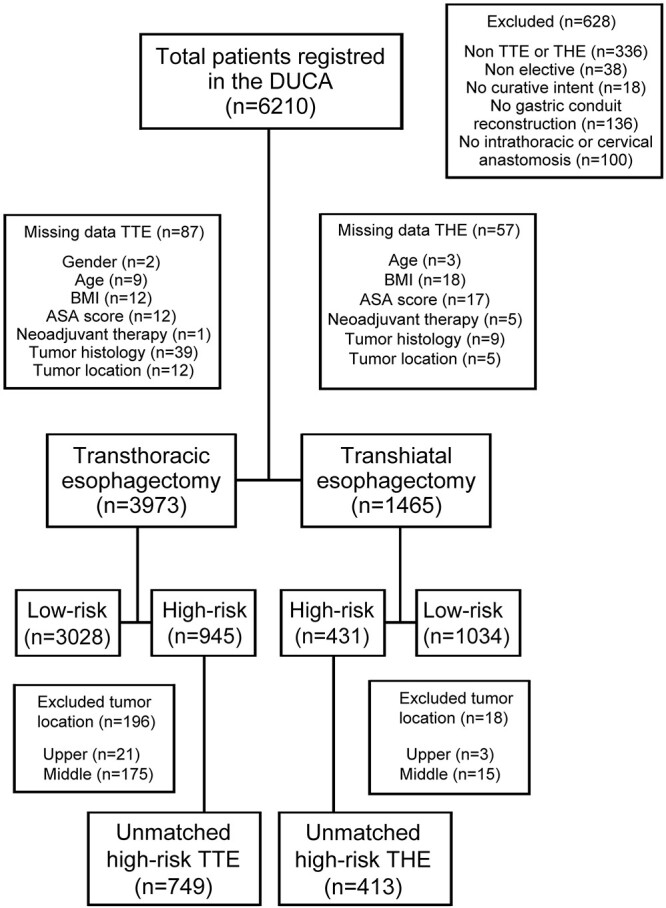
Transthoracic esophagectomy (TTE) for esophageal cancer facilitates mediastinal dissection; however, it has a significant impact on cardiopulmonary status. High-risk patients may therefore be better candidates for transhiatal esophagectomy (THE) in order to prevent serious complications. This study addressed short-term outcome following TTE and THE in patients that are considered to have a higher risk of surgery-related morbidity. This population-based study included patients who underwent a curative esophagectomy between 2011 and 2018, registered in the Dutch Upper GI Cancer Audit. The Charlson comorbidity index was used to assign patients to a low-risk (score ≤ 1) and high-risk group (score ≥ 2). Propensity score matching was applied to produce comparable groups between high-risk patients receiving TTE and THE. Primary endpoint was mortality (in-hospital/30-day mortality), secondary endpoints included morbidity and oncological outcomes. Additionally, a matched subgroup analysis was performed, including only cervical reconstructions. Of 5,438 patients, 945 and 431 high-risk patients underwent TTE and THE, respectively. After propensity score matching, mortality (6.3 vs 3.3%, P = 0.050), overall morbidity, Clavien-Dindo ≥ 3 complications, pulmonary complications, cardiac complications and re-interventions were significantly more observed after TTE compared to THE. A significantly higher mortality after TTE with a cervical reconstruction was found compared to THE (7.0 vs. 2.2%, P = 0.020). Patients with a high Charlson comorbidity index predispose for a complicated postoperative course after esophagectomy, this was more outspoken after TTE compared to THE. In daily practice, these outcomes should be balanced with the lower lymph node yield, but comparable positive node count and radicality after THE.
Keywords: Charlson comorbidity index; mortality; population-based; propensity score matching; transhiatal esophagectomy; transthoracic esophagectomy.
© The Author(s) 2022. Published by Oxford University Press on behalf of International Society for Diseases of the Esophagus.
Figures
References
-
- van Hagen P, Hulshof M C, van Lanschot J J et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med 2012; 366: 2074–84. - PubMed
-
- Hulscher J B F, van Sandick J W, de Boer A G E M et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. New England Journal of Medicine 2002; 347: 1662–9. - PubMed
-
- Peyre C G, Hagen J A, DeMeester S R et al. The number of lymph nodes removed predicts survival in esophageal cancer: an international study on the impact of extent of surgical resection. Ann Surg 2008; 248: 549–56. - PubMed
-
- Omloo J M, Lagarde S M, Hulscher J B et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the mid/distal esophagus: five-year survival of a randomized clinical trial. Ann Surg 2007; 246: 992–1000 discussion 1000-1001. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
