

Outcomes of in-hospital cardiac arrest among hospitals with and without telemedicine critical care
- PMID: 35724851
- PMCID: PMC9296566
- DOI: 10.1016/j.resuscitation.2022.06.008
Outcomes of in-hospital cardiac arrest among hospitals with and without telemedicine critical care
Abstract
Background: Survival rates following in-hospital cardiac arrest (IHCA) are lower during nights and weekends (off-hours), as compared to daytime on weekdays (on-hours). Telemedicine Critical Care (TCC) may provide clinical support to improve IHCA outcomes, particularly during off-hours.
Objective: To evaluate the association between hospital availability of TCC and IHCA survival.
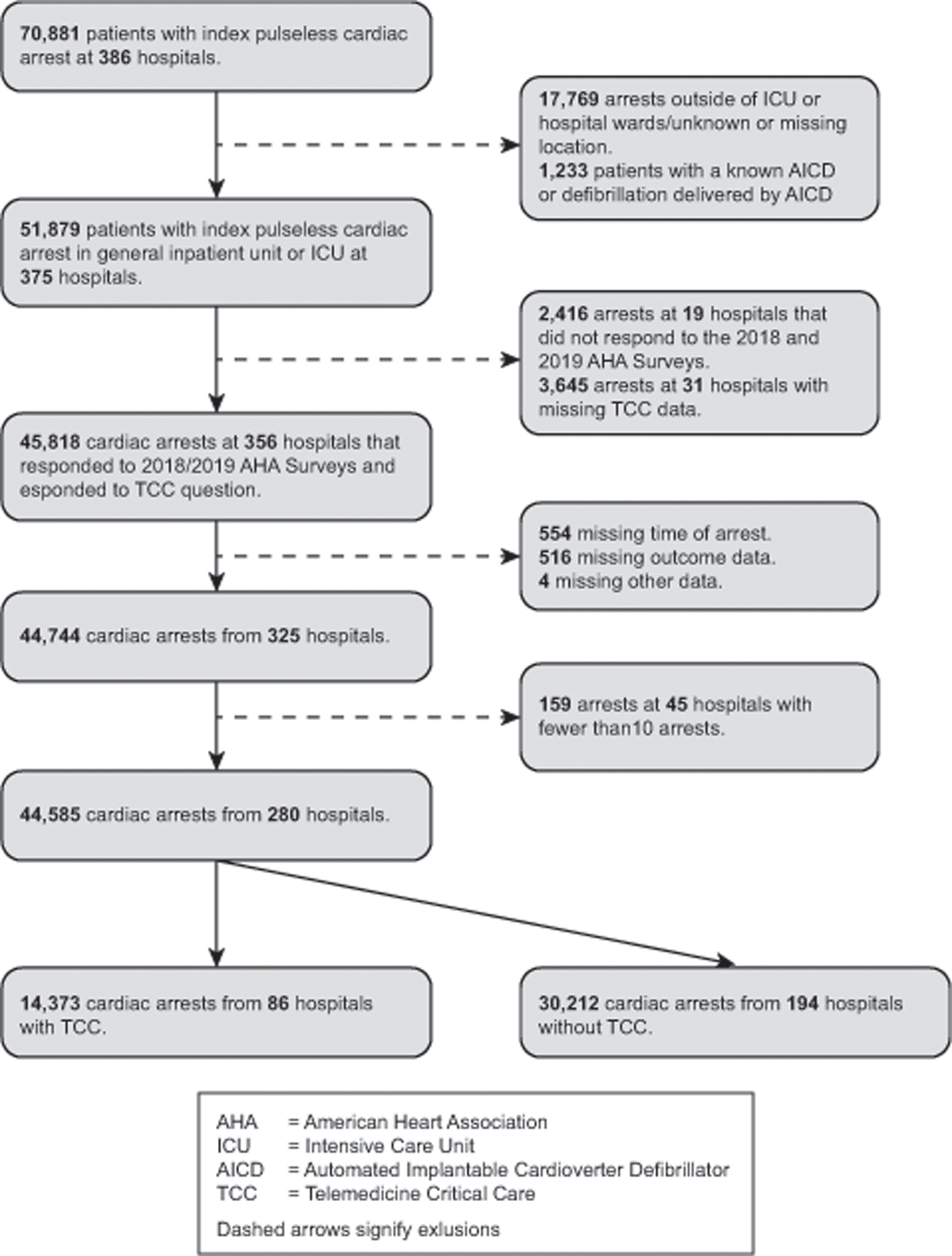
Methods: We identified 44,585 adults at 280 U.S. hospitals in the Get With The Guidelines® - Resuscitation registry who suffered IHCA in an Intensive Care Unit (ICU) or hospital ward between July 2017 and December 2019. We used 2-level hierarchical multivariable logistic regression to investigate whether TCC availability was associated with better survival, overall, and during on-hours (Monday-Friday 7:00 a.m.-10:59p.m.) vs. off-hours (Monday-Friday 11:00p.m.-6:59 a.m., and Saturday-Sunday, all day, and US national holidays).
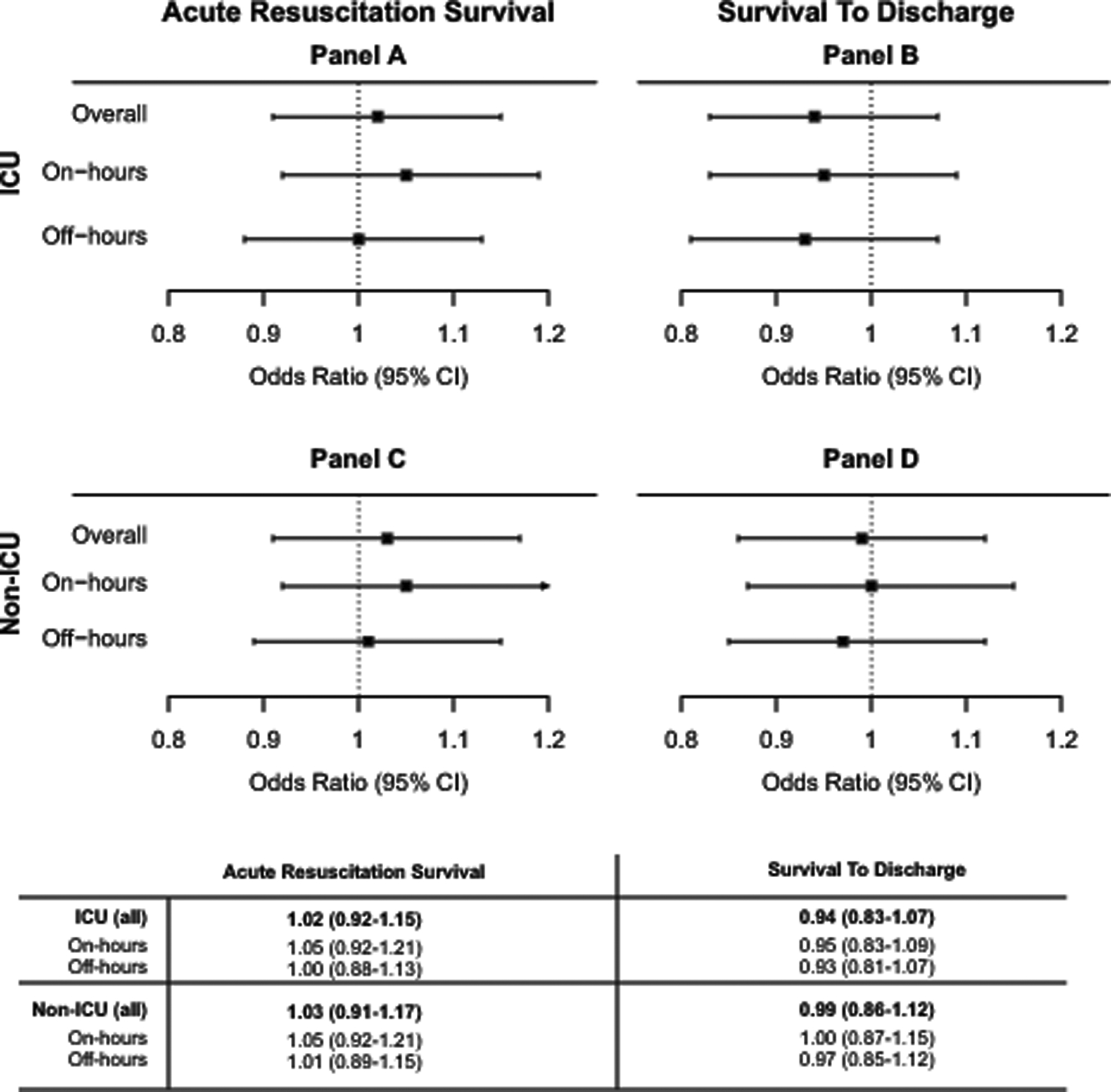
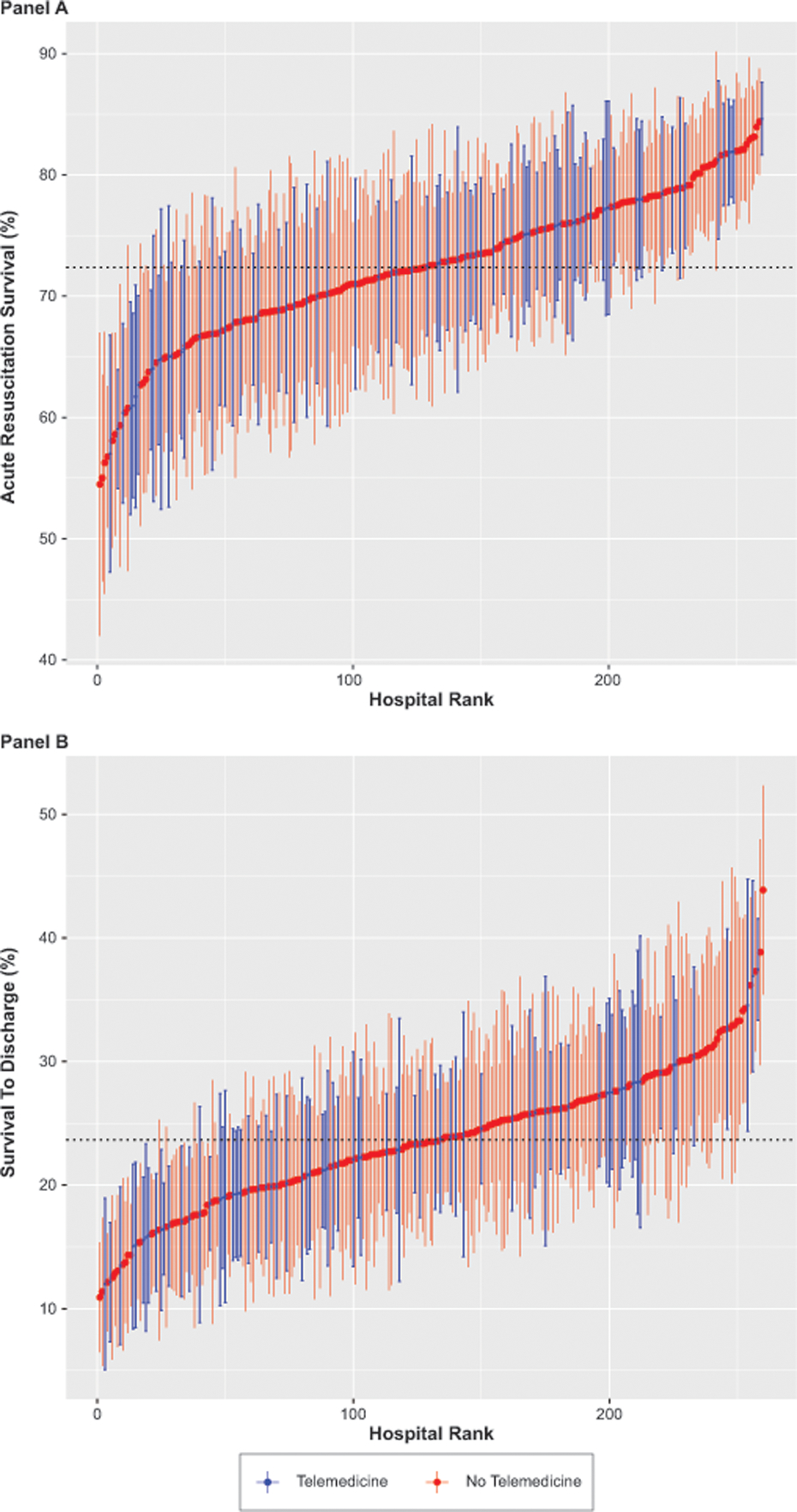
Results: 14,373 (32.2%) participants suffered IHCA at hospitals with TCC, and 27,032 (60.6%) occurred in an ICU. There was no difference between TCC and non-TCC hospitals in acute resuscitation survival rate or survival to discharge rates for either IHCA occurring in the ICU (acute survival odds ratio [OR] 1.02, 95% CI 0.92-1.15; survival to discharge OR 0.94 [0.83-1.07]) or outside of the ICU (acute survival OR 1.03 [0.91-1.17]; survival to discharge OR 0.99 [0.86-1.12]. Timing of cardiac arrest did not modify the association between TCC availability and acute resuscitation survival (P =.37 for interaction) or survival to discharge (P =.39 for interaction).
Conclusions: Hospital availability of TCC was not associated with improved outcomes for in-hospital cardiac arrest.
Keywords: Cardiopulmonary arrest; Cardiopulmonary resuscitation; Critical Care; Tele-Critical Care; Tele-ICU; Telehealth; Telemedicine.
Copyright © 2022 Elsevier B.V. All rights reserved.
Conflict of interest statement
CONFLICTS OF INTEREST
Dr. Joynt Maddox serves on the Health Policy Advisory Council for the Centene Corporation (St. Louis, MO). All other authors have declared no conflict of interest
All GWTG participating institutions were required to comply with local regulatory and privacy guidelines and, if required, to secure institutional review board approval. Because data were used primarily at the local site for quality improvement, sites were granted a waiver of informed consent under the common rule.
Figures
References
-
- Peberdy MA, Ornato JP, Larkin GL, et al. Survival from in-hospital cardiac arrest during nights and weekends. Jama. 2008;299(7):785–792. - PubMed
-
- Brady WJ, Gurka KK, Mehring B, Peberdy MA, O’Connor RE, American Heart Association’s Get with the Guidelines I. In-hospital cardiac arrest: impact of monitoring and witnessed event on patient survival and neurologic status at hospital discharge. Resuscitation. 2011;82(7):845–852. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
