

Kyoto international consensus report on anatomy, pathophysiology and clinical significance of the gastro-oesophageal junction
- PMID: 35725291
- PMCID: PMC9279854
- DOI: 10.1136/gutjnl-2022-327281
Kyoto international consensus report on anatomy, pathophysiology and clinical significance of the gastro-oesophageal junction
Abstract
Objective: An international meeting was organised to develop consensus on (1) the landmarks to define the gastro-oesophageal junction (GOJ), (2) the occurrence and pathophysiological significance of the cardiac gland, (3) the definition of the gastro-oesophageal junctional zone (GOJZ) and (4) the causes of inflammation, metaplasia and neoplasia occurring in the GOJZ.
Design: Clinical questions relevant to the afore-mentioned major issues were drafted for which expert panels formulated relevant statements and textural explanations.A Delphi method using an anonymous system was employed to develop the consensus, the level of which was predefined as ≥80% of agreement. Two rounds of voting and amendments were completed before the meeting at which clinical questions and consensus were finalised.
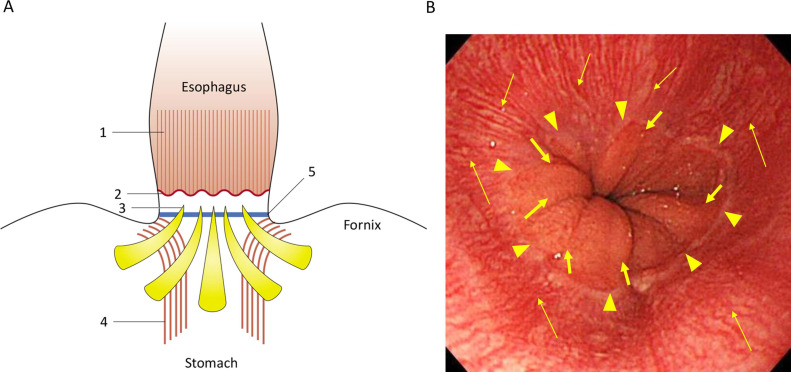
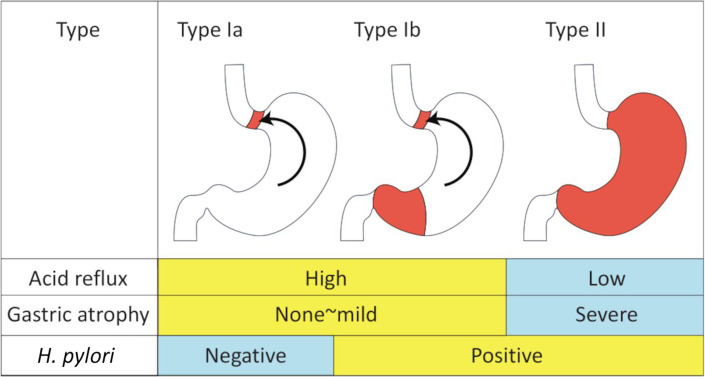
Results: Twenty eight clinical questions and statements were finalised after extensive amendments. Critical consensus was achieved: (1) definition for the GOJ, (2) definition of the GOJZ spanning 1 cm proximal and distal to the GOJ as defined by the end of palisade vessels was accepted based on the anatomical distribution of cardiac type gland, (3) chemical and bacterial (Helicobacter pylori) factors as the primary causes of inflammation, metaplasia and neoplasia occurring in the GOJZ, (4) a new definition of Barrett's oesophagus (BO).
Conclusions: This international consensus on the new definitions of BO, GOJ and the GOJZ will be instrumental in future studies aiming to resolve many issues on this important anatomic area and hopefully will lead to better classification and management of the diseases surrounding the GOJ.
Keywords: BARRETT'S CARCINOMA; BARRETT'S OESOPHAGUS; GASTRO-OESPHAGEAL JUNCTION; GASTROESOPHAGEAL REFLUX DISEASE; HELICOBACTER PYLORI.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KS serves as an advisor for Fujifilm Medical Co. and received a lecture fee from Fujifilm Medical Co. MF received lecture fee from Olympus Medical Systems Co. and Fujifilm Medical Co. He also received research grant from Olympus Medical Systems Co, Fujifilm Medical Co. and HOYA Pentax Co. HI serves as an advisor for Olympus Medical Systems Co. HM received a lecture fee from Fujifilm Medical Co. GT and HT received lecture fees from Olympus Medical Co. and Fujifilm Medical Co. Other authors have declared no competing interests regarding this manuscript
Figures
Similar articles
-
Cytokeratin immunoreactivity of intestinal metaplasia at normal oesophagogastric junction indicates its aetiology.Gut. 2001 Dec;49(6):761-6. doi: 10.1136/gut.49.6.761. Gut. 2001. PMID: 11709508 Free PMC article.
-
Review article: prevalence of Barrett's oesophagus and metaplasia at the gastro-oesophageal junction.Aliment Pharmacol Ther. 2004 Oct;20 Suppl 5:48-54; discussion 61-2. doi: 10.1111/j.1365-2036.2004.02138.x. Aliment Pharmacol Ther. 2004. PMID: 15456464 Review.
-
Asia-Pacific consensus on the management of gastro-oesophageal reflux disease: an update focusing on refractory reflux disease and Barrett's oesophagus.Gut. 2016 Sep;65(9):1402-15. doi: 10.1136/gutjnl-2016-311715. Epub 2016 Jun 3. Gut. 2016. PMID: 27261337
-
Cytokeratin 7 and 20 expression in intestinal metaplasia of the distal oesophagus: relationship to gastro-oesophageal reflux disease.Histopathology. 2005 Sep;47(3):268-75. doi: 10.1111/j.1365-2559.2005.02219.x. Histopathology. 2005. PMID: 16115227
-
Global prevalence of Barrett's oesophagus and oesophageal cancer in individuals with gastro-oesophageal reflux: a systematic review and meta-analysis.Gut. 2021 Mar;70(3):456-463. doi: 10.1136/gutjnl-2020-321365. Epub 2020 Jul 30. Gut. 2021. PMID: 32732370
Cited by
-
Cancer risk by length of Barrett's esophagus in Japanese population: a nationwide multicenter retrospective cohort study.J Gastroenterol. 2024 Oct;59(10):887-895. doi: 10.1007/s00535-024-02139-2. Epub 2024 Aug 16. J Gastroenterol. 2024. PMID: 39150527
-
Gastro-Esophageal Junction Precancerosis: Histological Diagnostic Approach and Pathogenetic Insights.Cancers (Basel). 2023 Dec 6;15(24):5725. doi: 10.3390/cancers15245725. Cancers (Basel). 2023. PMID: 38136271 Free PMC article. Review.
-
Usefulness of Endoscopy for the Detection and Diagnosis of Primary Esophageal Motility Disorders and Diseases Relating to Abnormal Esophageal Motility.Diagnostics (Basel). 2023 Feb 12;13(4):695. doi: 10.3390/diagnostics13040695. Diagnostics (Basel). 2023. PMID: 36832183 Free PMC article. Review.
-
UpFront.Frontline Gastroenterol. 2023 Jun 6;14(4):269-270. doi: 10.1136/flgastro-2023-102467. eCollection 2023. Frontline Gastroenterol. 2023. PMID: 37409328 Free PMC article. No abstract available.
-
Development of a prediction score for Barrett's esophagus in Japanese health checkup settings.Esophagus. 2024 Oct;21(4):552-562. doi: 10.1007/s10388-024-01079-3. Epub 2024 Aug 19. Esophagus. 2024. PMID: 39158677