

Postoperative morbidity and health-related quality of life in children with delayed reconstruction of esophageal atresia: a nationwide Swedish study
- PMID: 35725462
- PMCID: PMC9207832
- DOI: 10.1186/s13023-022-02381-y
Postoperative morbidity and health-related quality of life in children with delayed reconstruction of esophageal atresia: a nationwide Swedish study
Abstract
Background: In 10-15% of children with esophageal atresia (EA) delayed reconstruction of esophageal atresia (DREA) is necessary due to long-gap EA and/or prematurity/low birth weight. They represent a patient subgroup with high risk of complications. We aimed to evaluate postoperative morbidity and health-related quality of life (HRQOL) in a Swedish national cohort of children with DREA.
Methods: Postoperative morbidity, age-specific generic HRQOL (PedsQL™ 4.0) and condition-specific HRQOL (The EA-QOL questionnaires) in children with DREA were compared with children with EA who had primary anastomosis (PA). Factors associated with the DREA group's HRQOL scores were analyzed using Mann-Whitney U-test and Spearman's rho. Clinical data was extracted from the medical records. Significance level was p < 0.05.
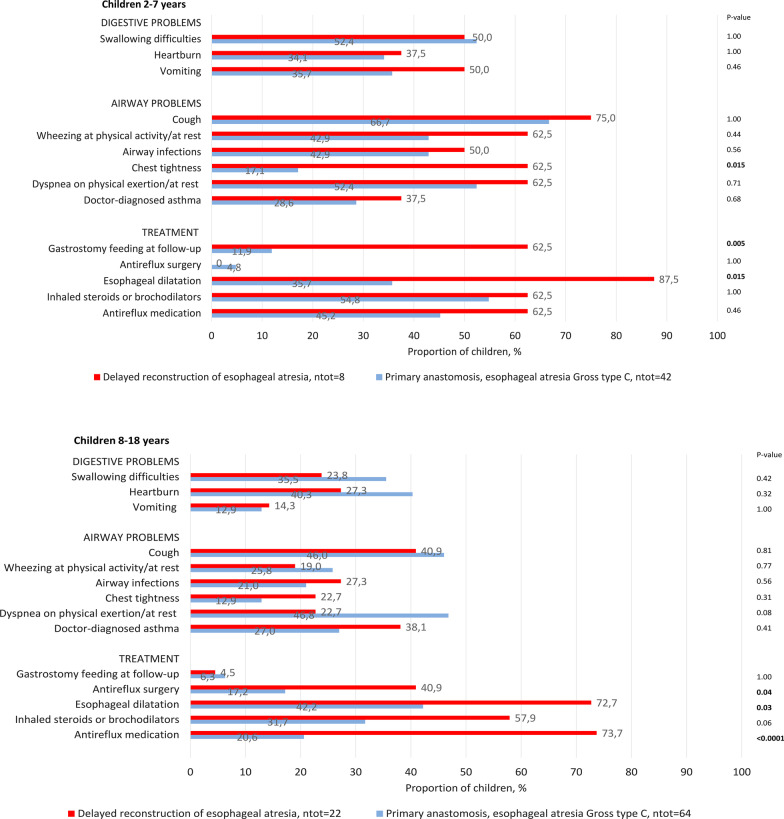
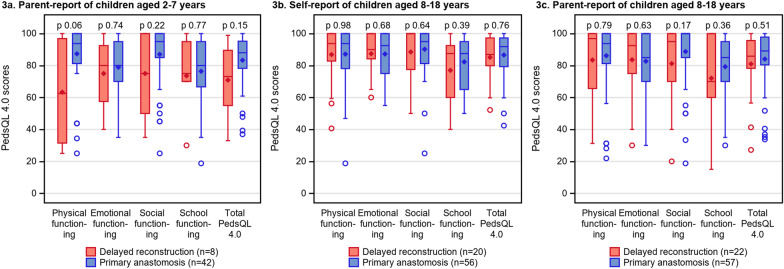
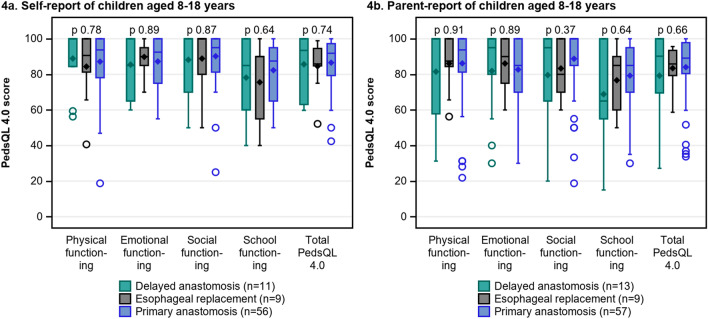
Results: Thirty-four out of 45 families of children with DREA were included and 30 returned the questionnaires(n = 8 children aged 2-7 years; n = 22 children aged 8-18 years). Compared to children with PA(42 children aged 2-7 years; 64 children aged 8-18 years), there were no significant differences in most early postoperative complications. At follow-up, symptom prevalence in children aged 2-7 with DREA ranged from 37.5% (heartburn) to 75% (cough). Further digestive and respiratory symptoms were present in ≥ 50%. In children aged 8-18, it ranged from 14.3% (vomiting) to 40.9% (cough), with other digestive and airway symptoms present in 19.0-27.3%. Except for chest tightness (2-7 years), there were no significant differences in symptom prevalence between children with DREA and PA, nor between their generic or condition-specific HRQOL scores (p > 0.05). More children with DREA underwent esophageal dilatations (both age groups), gastrostomy feeding (2-7 years), and antireflux treatment (8-18 years), p < 0.05. Days to hospital discharge after EA repair and a number of associated anomalies showed a strong negative correlation with HRQOL scores (2-7 years). Presence of cough, airway infection, swallowing difficulties and heartburn were associated with lower HRQOL scores (8-18 years), p < 0.05.
Conclusions: Although children with DREA need more treatments, they are not a risk group for postoperative morbidity and impaired HRQOL compared with children with PA. However, those with a long initial hospital stay, several associated anomalies and digestive or respiratory symptoms risk worse HRQOL. This is important information for clinical practice, families and patient stakeholders.
Keywords: Delayed reconstruction; Esophageal atresia; Health-related quality of life; Long-gap esophageal atresia; Long-term morbidity; Postoperative outcomes.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Clinical Factors Affecting Condition-Specific Quality-of-Life Domains in Pediatric Patients after Repair of Esophageal Atresia: The Swedish-German EA-QOL Study.Eur J Pediatr Surg. 2020 Feb;30(1):96-103. doi: 10.1055/s-0039-1693729. Epub 2019 Jul 25. Eur J Pediatr Surg. 2020. PMID: 31344708
-
Prevalence and risk factors of feeding difficulties in children with delayed reconstruction of esophageal atresia: a Swedish nationwide study.Pediatr Surg Int. 2025 Jun 11;41(1):164. doi: 10.1007/s00383-025-06052-4. Pediatr Surg Int. 2025. PMID: 40498126 Free PMC article.
-
Prevalence of Mental Health Problems, Associated Factors, and Health-Related Quality of Life in Children with Long-Gap Esophageal Atresia in Sweden.J Pediatr Surg. 2023 Sep;58(9):1646-1655. doi: 10.1016/j.jpedsurg.2022.12.004. Epub 2022 Dec 15. J Pediatr Surg. 2023. PMID: 36635161
-
Health-Related Quality of Life in Patients after Repair of Esophageal Atresia: A Review of Current Literature.Eur J Pediatr Surg. 2020 Jun;30(3):239-250. doi: 10.1055/s-0040-1710389. Epub 2020 May 29. Eur J Pediatr Surg. 2020. PMID: 32483796 Review.
-
Health-related quality of life among children, young people and adults with esophageal atresia: a review of the literature and recommendations for future research.Qual Life Res. 2015 Oct;24(10):2433-45. doi: 10.1007/s11136-015-0975-x. Epub 2015 Apr 1. Qual Life Res. 2015. PMID: 25829227 Review.
Cited by
-
Clinical outcome, quality of life, and mental health in long-gap esophageal atresia: comparison of gastric sleeve pull-up and delayed primary anastomosis.Pediatr Surg Int. 2023 Apr 4;39(1):166. doi: 10.1007/s00383-023-05448-4. Pediatr Surg Int. 2023. PMID: 37014441 Free PMC article.
-
Management of long-gap esophageal atresia.Transl Pediatr. 2024 Feb 29;13(2):329-342. doi: 10.21037/tp-23-453. Epub 2024 Feb 27. Transl Pediatr. 2024. PMID: 38455743 Free PMC article. Review.
-
Parents' experiences of sham feeding their child with esophageal atresia at home while awaiting reconstructive surgery. A qualitative interview study.Pediatr Surg Int. 2024 Feb 29;40(1):61. doi: 10.1007/s00383-024-05660-w. Pediatr Surg Int. 2024. PMID: 38421506 Free PMC article.
-
Schooling experiences in children with long-gap esophageal atresia compared with children with esophageal atresia and primary anastomosis: a Swedish study.Orphanet J Rare Dis. 2023 Aug 7;18(1):233. doi: 10.1186/s13023-023-02846-8. Orphanet J Rare Dis. 2023. PMID: 37550744 Free PMC article.
-
Experiences of symptom burden among young children born with esophageal atresia-tracheoesophageal fistula: a US focus group study.Orphanet J Rare Dis. 2025 Aug 18;20(1):438. doi: 10.1186/s13023-025-03939-2. Orphanet J Rare Dis. 2025. PMID: 40826120 Free PMC article.
References
-
- Pedersen RN, Calzolari E, Husby S, Garne E. Oesophageal atresia: prevalence, prenatal diagnosis and associated anomalies in 23 European regions. Arch Dis Child. 2012;97(3):227–232. - PubMed
-
- Zimmer J, Eaton S, Murchison LE, De Coppi P, Ure BM, Dingemann C. State of play: eight decades of surgery for esophageal atresia. Eur J Pediatr Surg. 2019;29(1):39–48. - PubMed
-
- Baird R, Lal DR, Ricca RL, Diefenbach KA, Downard CD, Shelton J, et al. Management of long gap esophageal atresia: a systematic review and evidence-based guidelines from the APSA outcomes and evidence based practice committee. J Pediatr Surg. 2019;54(4):675–687. - PubMed
-
- Zani A, Wolinska J, Cobellis G, Chiu PP, Pierro A. Outcome of esophageal atresia/tracheoesophageal fistula in extremely low birth weight neonates (<1000 grams) Pediatr Surg Int. 2016;32(1):83–88. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
