

Massive adrenocortical carcinoma presenting as peripheral edema: a case report
- PMID: 35725572
- PMCID: PMC9210600
- DOI: 10.1186/s13256-022-03397-5
Massive adrenocortical carcinoma presenting as peripheral edema: a case report
Abstract
Background: Adrenocortical carcinoma is a rare, but potentially lethal, malignancy that is usually detected as an incidental finding on abdominal imaging studies or owing to hormonal complications. This report recounts an unusual presentation with leg edema due to compression of the inferior vena cava. The dearth of proven effective treatment is also addressed.
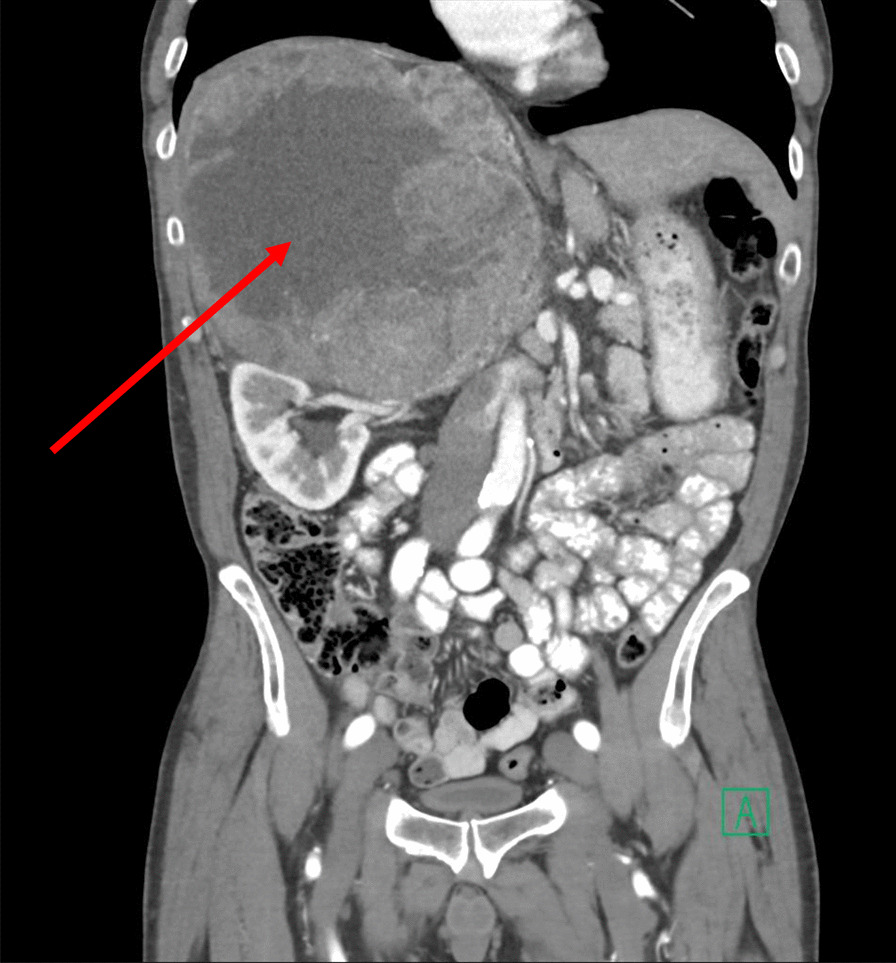
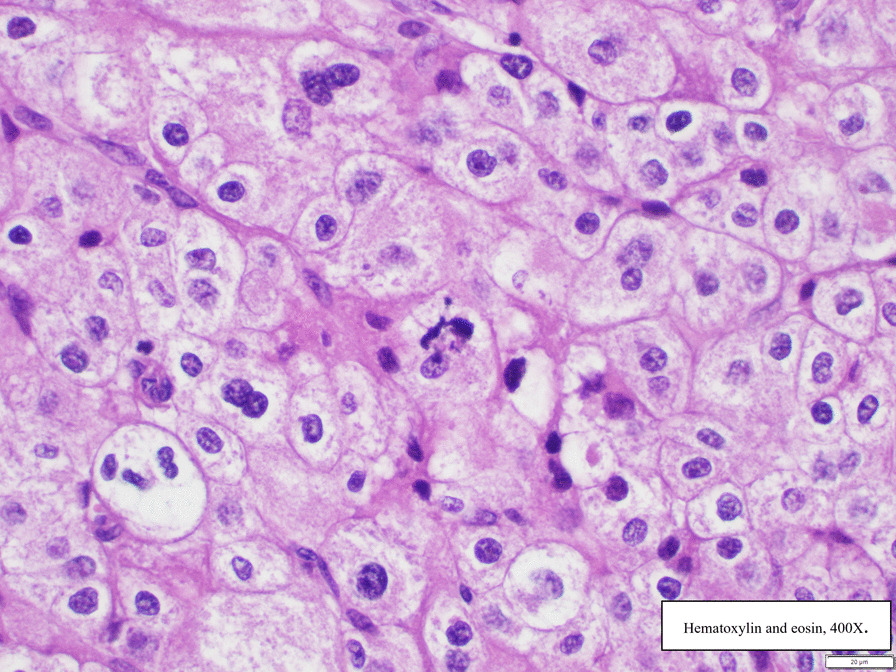
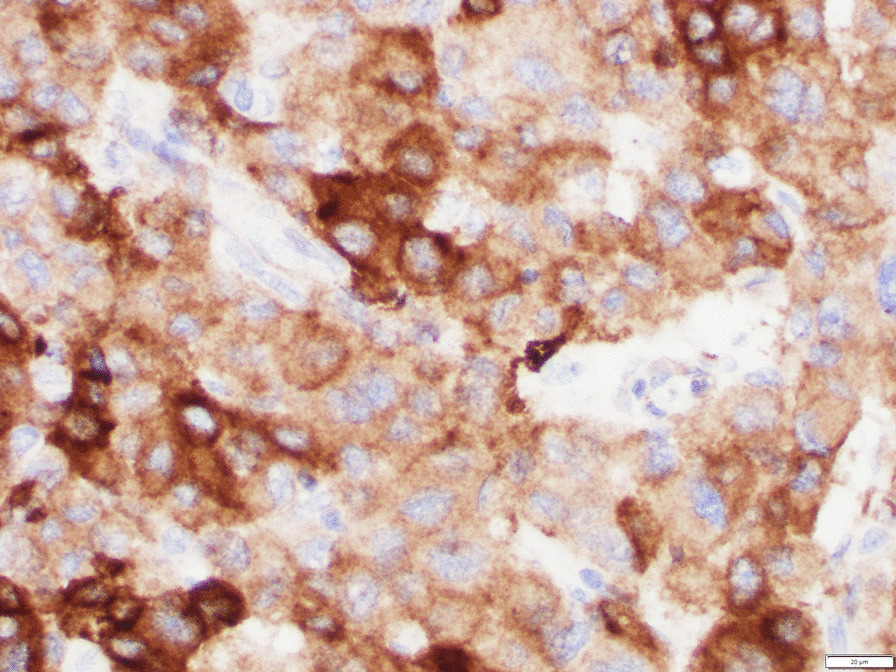
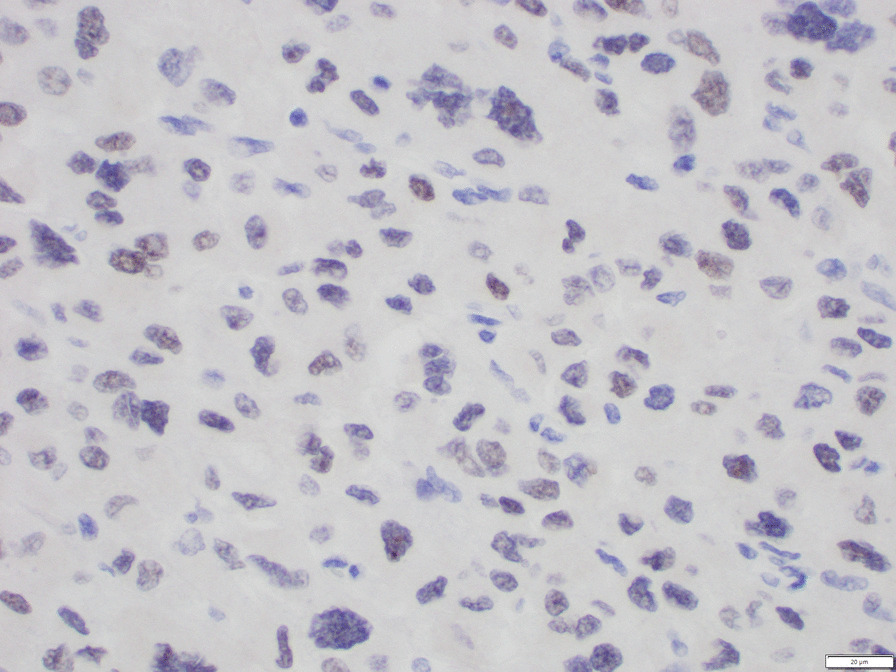
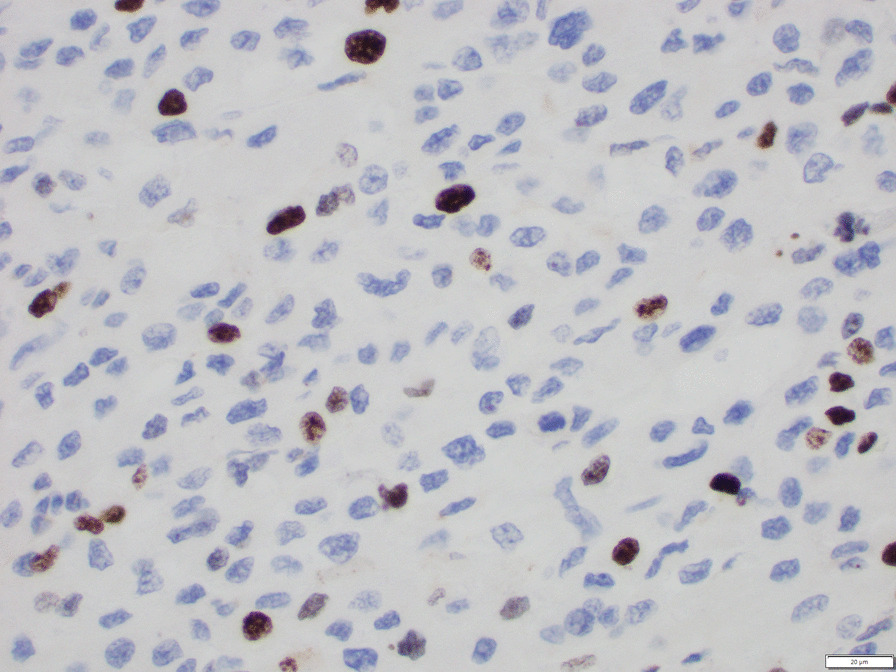
Case presentation: A 65-year-old White male physician presented with severe, bilateral pitting edema that extended from the toes to the thighs. It progressed over several months. He also experienced paroxysmal dyspnea. Evaluation of cardiac, hepatic, and renal function failed to determine a cause. Computed tomography revealed a tumor above the right kidney, with compression of the intrahepatic inferior vena cava and upstream distension. Serum cortisol and dehydroepiandrosterone sulfate concentrations were elevated, 24-hour urinary cortisol level was elevated, and serum adrenocorticotropic hormone and testosterone concentrations were suppressed. A 27-cm tumor, the right lobe of the liver, the right kidney, and 26 lymph nodes were resected. Histological study confirmed the diagnosis of adrenocortical carcinoma. Ki67 proliferation index was 26.7% (worse prognosis associated with index > 10%). Lymph nodes were negative for malignancy, but a separate 2.7-cm tumor was found near the renal hilum. Adjuvant mitotane chemotherapy was prescribed. Serum testosterone concentration returned to normal. High-dose hydrocortisone administration was needed because of adrenal suppression and CYP 3A4 induction by mitotane.
Conclusion: Imaging of the abdomen and pelvis should be conducted in cases of unexplained leg edema. In this case, a large adrenal cancer compressed the vena cava. Iron deficiency followed resection of the large tumor. Advanced stages of adrenocortical carcinoma are associated with poor prognosis. Mitotane chemotherapy is a standard but unproven adjuvant treatment that is associated with many complications, and its induction of hepatic CYP 3A4 enzymes necessitates adjustment of other medications.
Keywords: Adrenocortical carcinoma; Ki67 index; Mitotane; Peripheral edema.
© 2022. The Author(s).
Conflict of interest statement
The author declares that he has no competing interests.
Figures

References
-
- Braunwald E, Loscalzo J. Edema. In: Jameson JL, Fauci AS, Kasper, et al, editors. Harrison’s principles of internal medicine. 20th ed. New York: McGraw-Hill Education; 2018. p. 237–40.
-
- Skorecki KL, Winaver J, Abassi ZA. Extracellular fluid and edema formation. In: Brenner BM, editor. Brenner & Rector’s The Kidney. 8. Philadelphia: Saunders Elsevier; 2008. pp. 398–458.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
