

Biological factors that may impair transplacental transfer of RSV antibodies: Implications for maternal immunization policy and research priorities for low- and middle-income countries
- PMID: 35725783
- PMCID: PMC9348036
- DOI: 10.1016/j.vaccine.2022.06.034
Biological factors that may impair transplacental transfer of RSV antibodies: Implications for maternal immunization policy and research priorities for low- and middle-income countries
Abstract
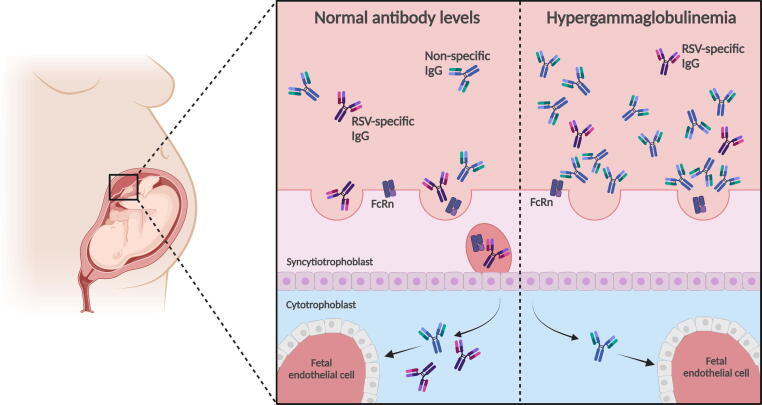
Respiratory syncytial virus (RSV) is the leading viral cause of acute lower respiratory tract infection (ALRI), including bronchiolitis and pneumonia, in infants and children worldwide. Protection against RSV is primarily antibody mediated and passively acquired RSV neutralizing antibody can protect infants from RSV ALRI. Maternal immunization is an attractive strategy for the prevention of RSV in early infancy when immune responses to active immunization may be suboptimal and most severe RSV disease and death occur. However, several biologic factors have been shown to potentially attenuate or interfere with the transfer of protective naturally acquired antibodies from mother to fetus and could therefore also reduce vaccine effectiveness through impairment of transfer of vaccine-induced antibodies. Many of these factors are prevalent in low- and middle-income countries (LMIC) which experience the greatest burden of RSV-associated mortality; more data are needed to understand these mechanisms in the context of RSV maternal immunization. This review will focus on what is currently known about biologic conditions that may impair RSV antibody transfer, including preterm delivery, low birthweight, maternal HIV infection, placental malaria, and hypergammaglobulinemia (high levels of maternal total IgG). Key data gaps and priority areas for research are highlighted and include improved understanding of the epidemiology of hypergammaglobulinemia and the mechanisms by which it may impair antibody transfer. Key considerations for ensuring optimal vaccine effectiveness in LMICs are also discussed.
Keywords: Hypergammaglobulinemia; Maternal immunization; Passive immunization; Respiratory syncytial virus; Transplacental antibody transport.
Copyright © 2022. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Shi T., McAllister D.A., O'Brien K.L., Simoes E.A.F., Madhi S.A., Gessner B.D., et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390:946–958. - PMC - PubMed
-
- Singleton R., Dooley L., Bruden D., Raelson S., Butler J.C. Impact of palivizumab prophylaxis on respiratory syncytial virus hospitalizations in high risk Alaska Native infants. Pediatr Infect Dis J. 2003;22:540–545. - PubMed
-
- Glezen W.P., Taber L.H., Frank A.L., Kasel J.A. Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Child. 1960;1986(140):543–546. - PubMed
-
- Groothuis J.R., Simoes E.A., Levin M.J., Hall C.B., Long C.E., Rodriguez W.J., et al. Prophylactic administration of respiratory syncytial virus immune globulin to high-risk infants and young children. The Respiratory Syncytial Virus Immune Globulin Study Group. N Engl J Med. 1993;329:1524–1530. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
