

β-blockers and breast cancer survival by molecular subtypes: a population-based cohort study and meta-analysis
- PMID: 35725814
- PMCID: PMC9470740
- DOI: 10.1038/s41416-022-01891-7
β-blockers and breast cancer survival by molecular subtypes: a population-based cohort study and meta-analysis
Abstract
Background: The association between use of β-blockers and breast cancer (BC) prognosis has been investigated in several observational studies, with conflicting results. We performed a nationwide cohort study and a meta-analysis to investigate the association, and assess if it varied between molecular subtypes of BC.
Methods: We identified women aged ≥50 years with BC diagnosed between 2004 and 2018 in Norway. We used Cox regression models to estimate the association between β-blocker use at diagnosis and BC-specific survival, overall and by molecular subtype. We performed a meta-analysis of observational studies that reported molecular subtype-specific estimates of this association.
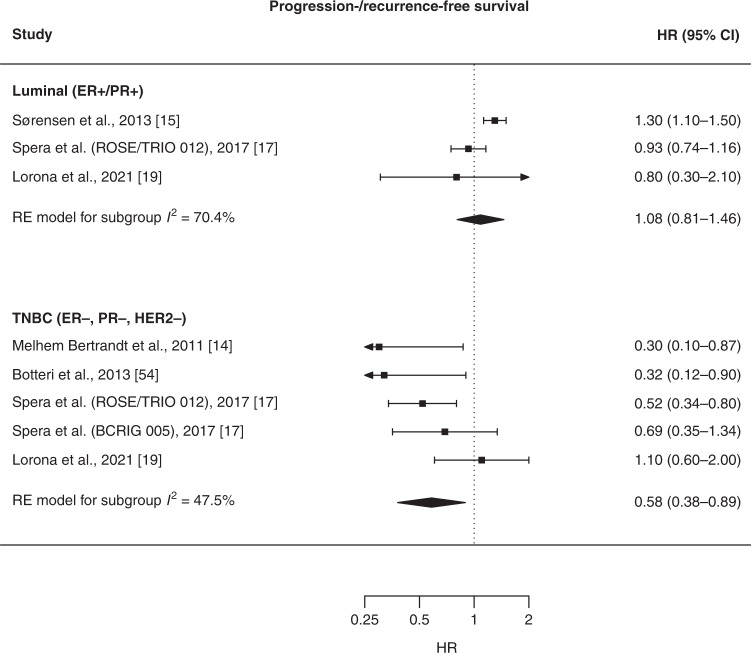
Results: We included 30,060 women, of which 4461 (15%) used β-blockers. After a median follow-up of 5.1 years, 2826 (9%) died of BC. Overall, β-blocker use was not associated with BC-specific survival (hazard ratio [HR] = 1.07; 95% confidence interval [CI]: 0.97-1.19). We found an association only in triple-negative BC (TNBC) patients (HR = 0.66; 95% CI: 0.47-0.91). This was confirmed in the meta-analysis: β-blocker use was associated with progression/recurrence-free (HR = 0.58; 95% CI: 0.38-0.89) and BC-specific survival (HR = 0.74; 95% CI: 0.55-1.00) in TNBC patients only.
Conclusion: In our cohort of BC patients and in the meta-analysis, β-blocker use was associated with prolonged BC-specific survival only in TNBC patients.
© 2022. The Author(s).
Conflict of interest statement
ES is a scientific advisory board member for Cygnal Therapeutics. The other authors have no competing interests.
Figures



References
-
- Cancer Registry of Norway. Cancer in Norway 2020—Cancer incidence, mortality, survival and prevalence in Norway. Oslo, Norway: Caner Registry of Norway; 2021.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
