Multispecies Probiotic for the Prevention of Antibiotic-Associated Diarrhea in Children: A Randomized Clinical Trial
- PMID: 35727573
- PMCID: PMC9214631
- DOI: 10.1001/jamapediatrics.2022.1973
Multispecies Probiotic for the Prevention of Antibiotic-Associated Diarrhea in Children: A Randomized Clinical Trial
Erratum in
-
Errors in Abstract and Text.JAMA Pediatr. 2022 Sep 1;176(9):948. doi: 10.1001/jamapediatrics.2022.2527. JAMA Pediatr. 2022. PMID: 35788632 Free PMC article. No abstract available.
Abstract
Importance: The efficacy of multispecies probiotic formulations in the prevention of antibiotic-associated diarrhea (AAD) remains unclear.
Objective: To assess the effect of a multispecies probiotic on the risk of AAD in children.
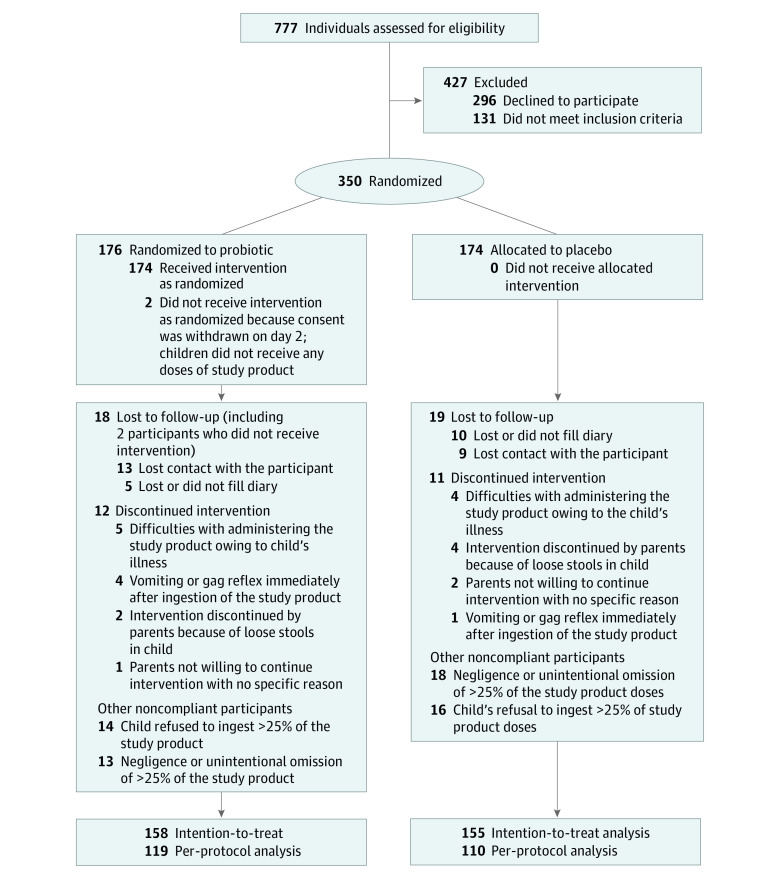
Design, setting, and participants: This randomized, quadruple-blind, placebo-controlled trial was conducted from February 2018 to May 2021 in a multicenter, mixed setting (inpatients and outpatients). Patients were followed up throughout the intervention period. Eligibility criteria included age 3 months to 18 years, recruitment within 24 hours following initiation of broad-spectrum systemic antibiotics, and signed informed consent. In total, 646 eligible patients were approached and 350 patients took part in the trial.
Interventions: A multispecies probiotic consisting of Bifidobacterium bifidum W23, Bifidobacterium lactis W51, Lactobacillus acidophilus W37, L acidophilus W55, Lacticaseibacillus paracasei W20, Lactiplantibacillus plantarum W62, Lacticaseibacillus rhamnosus W71, and Ligilactobacillus salivarius W24, for a total dose of 10 billion colony-forming units daily, for the duration of antibiotic treatment and for 7 days after.
Main outcomes and measures: The primary outcome was AAD, defined as 3 or more loose or watery stools per day in a 24-hour period, caused either by Clostridioides difficile or of otherwise unexplained etiology, after testing for common diarrheal pathogens. The secondary outcomes included diarrhea regardless of the etiology, diarrhea duration, and predefined diarrhea complications.
Results: A total of 350 children (192 boys and 158 girls; mean [range] age, 50 [3-212] months) were randomized and 313 were included in the intention-to-treat analysis. Compared with placebo (n = 155), the probiotic (n = 158) had no effect on risk of AAD (relative risk [RR], 0.81; 95% CI, 0.49-1.33). However, children in the probiotic group had a lower risk of diarrhea regardless of the etiology (RR, 0.65; 95% CI, 0.44-0.94). No differences were observed between the groups for most of the secondary outcomes, including adverse events.
Conclusions and relevance: A multispecies probiotic did not reduce the risk of AAD in children when analyzed according to the most stringent definition. However, it reduced the overall risk of diarrhea during and for 7 days after antibiotic treatment. Our study also shows that the AAD definition has a significant effect on clinical trial results and their interpretation.
Trial registration: ClinicalTrials.gov Identifier: NCT03334604.