

Digitally Delivered Exercise and Education Treatment Program for Low Back Pain: Longitudinal Observational Cohort Study
- PMID: 35727622
- PMCID: PMC9257621
- DOI: 10.2196/38084
Digitally Delivered Exercise and Education Treatment Program for Low Back Pain: Longitudinal Observational Cohort Study
Abstract
Background: Exercise and education is recommended as first-line treatment by evidence-based, international guidelines for low back pain (LBP). Despite consensus regarding the treatment, there is a gap between guidelines and what is offered to patients. Digital LBP treatments are an emerging way of delivering first-line treatment.
Objective: The aim of this study is to evaluate outcomes after participation in a 3-month digitally delivered treatment program for individuals with subacute or chronic LBP.
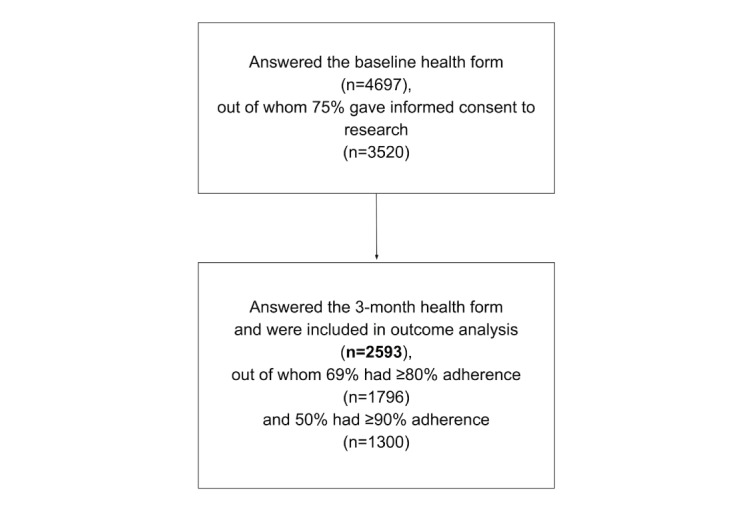
Methods: We analyzed data from 2593 consecutively recruited participants in a digitally delivered treatment program, available via the national health care system in Sweden. The program consists of video-instructed and progressive adaptable exercises, education through text lessons, and a chat and video function connecting participants with a personal physiotherapist. The primary outcome was mean change and proportion reaching a minimal clinically important change (MCIC) for LBP (2 points or 30% decrease) assessed with the numerical rating scale (average pain during the past week, discrete boxes, 0-10, best to worst). Secondary outcomes were mean change and proportion reaching MCIC (10 points or 30%) in disability, assessed with the Oswestry Disability Index (ODI; 0-100, best to worst) and a question on patient acceptable symptom state (PASS).
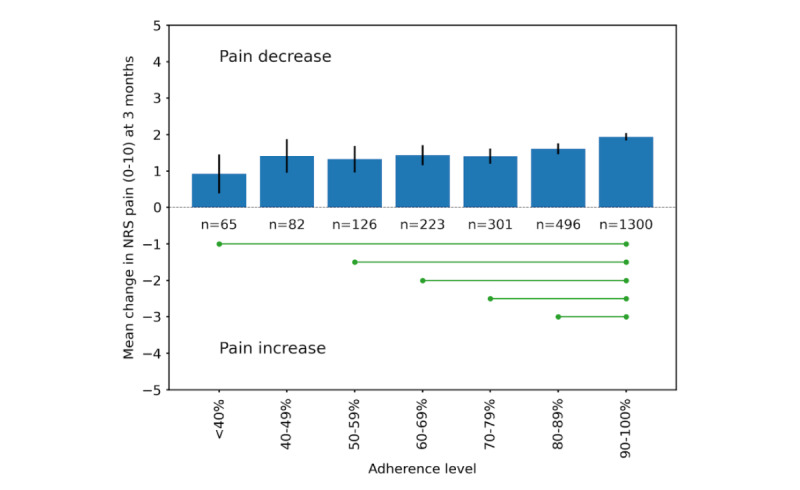
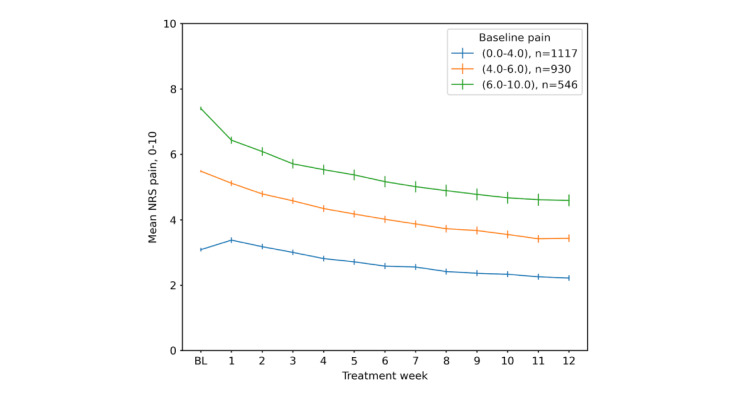
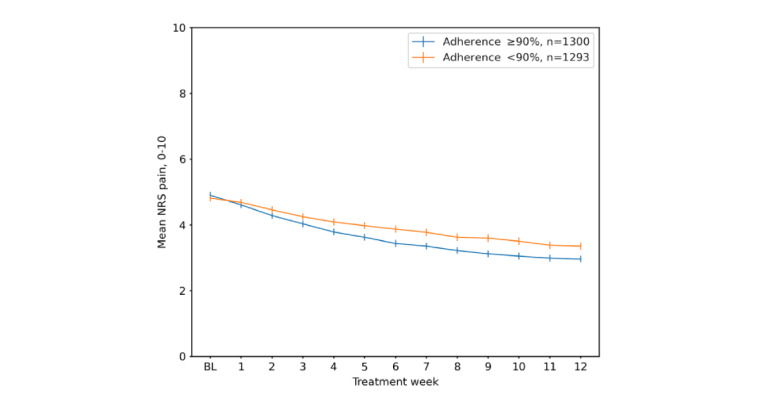
Results: The mean participant age was 63 years, 73.85% (1915/2593) were female, 54.72% (1419/2593) had higher education, 50.56% (1311/2593) were retired, and the mean BMI was 26.5 kg/m2. Participants completed on average 84% of the prescribed exercises and lessons, with an adherence of ≥80% in 69.26% (1796/2593) and ≥90% in 50.13% (1300/2593) of the participants. Mean reduction in pain from baseline to 3 months was 1.7 (95% CI -1.8 to -1.6), corresponding to a 35% relative change. MCIC was reached by 58.50% (1517/2593) of participants. ODI decreased 4 points (95% CI -4.5 to -3.7), and 36.48% (946/2593) reached an MCIC. A change from no to yes in PASS was seen in 30.35% (787/2593) of participants. Multivariable analysis showed positive associations between reaching an MCIC in pain and high baseline pain (odds ratio [OR] 1.9, 95% CI 1.6-2.1), adherence (OR 1.5, 95% CI 1.3-1.8), and motivation (OR 1.2, 95% CI 1.0-1.5), while we found negative associations for wish for surgery (OR 0.6, 95% CI 0.5-0.9) and pain in other joints (OR 0.9, 95% CI 0.7-0.9). We found no associations between sociodemographic characteristics and pain reduction.
Conclusions: Participants in this digitally delivered treatment for LBP had reduced pain at 3-month follow-up, and 58.50% (1517/2593) reported an MCIC in pain. Our findings suggest that digital treatment programs can reduce pain at clinically important levels for people with high adherence to treatment but that those with such severe LBP problems that they wish to undergo surgery may benefit from additional support.
Trial registration: ClinicalTrials.gov NCT05226156; https://clinicaltrials.gov/ct2/show/NCT05226156.
Keywords: back pain; chronic pain; digital care; digital therapy; exercise; health outcome; low back pain; pain management; physiotherapy; rehabilitation; telehealth; telemedicine.
©Helena Hörder, Håkan Nero, Majda Misini Ignjatovic, Ali Kiadaliri, L Stefan Lohmander, Leif E Dahlberg, Allan Abbott. Originally published in JMIR Rehabilitation and Assistive Technology (https://rehab.jmir.org), 21.06.2022.
Conflict of interest statement
Conflicts of Interest: HH, AK, and LSL are part-time employed by Joint Academy (JA); LED is the founder and chief medical officer at JA; HN is the vice president of clinical strategy at JA; MMI is full-time employed by JA as a data analyst. AA was a reviewer in the development of the content for the digital treatment program but received no compensation.
Figures
References
-
- Chen S, Chen M, Wu X, Lin S, Tao C, Cao H, Shao Z, Xiao G. Global, regional and national burden of low back pain 1990-2019: A systematic analysis of the Global Burden of Disease study 2019. J Orthop Translat. 2022 Jan;32:49–58. doi: 10.1016/j.jot.2021.07.005. https://linkinghub.elsevier.com/retrieve/pii/S2214-031X(21)00059-0 S2214-031X(21)00059-0 - DOI - PMC - PubMed
-
- Kreiner D, Matz P, Bono C, Cho Charles H, Easa John E, Ghiselli Gary, Ghogawala Zoher, Reitman Charles A, Resnick Daniel K, Watters William C, Annaswamy Thiru M, Baisden Jamie, Bartynski Walter S, Bess Shay, Brewer Randall P, Cassidy R Carter, Cheng David S, Christie Sean D, Chutkan Norman B, Cohen Bernard Allan, Dagenais Simon, Enix Dennis E, Dougherty Paul, Golish S Raymond, Gulur Padma, Hwang Steven W, Kilincer Cumhur, King Jeffrey A, Lipson Adam C, Lisi Anthony J, Meagher Richard J, O'Toole John E, Park Paul, Pekmezci Murat, Perry Daniel R, Prasad Ravi, Provenzano David A, Radcliff Kris E, Rahmathulla Gazanfar, Reinsel Tom E, Rich Robert L, Robbins Daniel S, Rosolowski Karie A, Sembrano Jonathan N, Sharma Anil K, Stout Alison A, Taleghani Christopher K, Tauzell Ryan A, Trammell Terry, Vorobeychik Yakov, Yahiro Amy M. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of low back pain. Spine J. 2020 Jul;20(7):998–1024. doi: 10.1016/j.spinee.2020.04.006.S1529-9430(20)30141-8 - DOI - PubMed
-
- Abbott Allan, Schröder Karin, Enthoven Paul, Nilsen Per, Öberg Birgitta. Effectiveness of implementing a best practice primary healthcare model for low back pain (BetterBack) compared with current routine care in the Swedish context: an internal pilot study informed protocol for an effectiveness-implementation hybrid type 2 trial. BMJ Open. 2018 Apr 24;8(4):e019906. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=29691246 bmjopen-2017-019906 - PMC - PubMed
-
- Schröder Karin, Öberg Birgitta, Enthoven P, Hedevik H, Fors M, Abbott A. Effectiveness and Quality of Implementing a Best Practice Model of Care for Low Back Pain (BetterBack) Compared with Routine Care in Physiotherapy: A Hybrid Type 2 Trial. J Clin Med. 2021 Mar 16;10(6):e1230. doi: 10.3390/jcm10061230. https://www.mdpi.com/resolver?pii=jcm10061230 jcm10061230 - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
