

Phase I study of adjuvant immunotherapy with autologous tumor-infiltrating lymphocytes in locally advanced cervical cancer
- PMID: 35727633
- PMCID: PMC9337833
- DOI: 10.1172/JCI157726
Phase I study of adjuvant immunotherapy with autologous tumor-infiltrating lymphocytes in locally advanced cervical cancer
Abstract
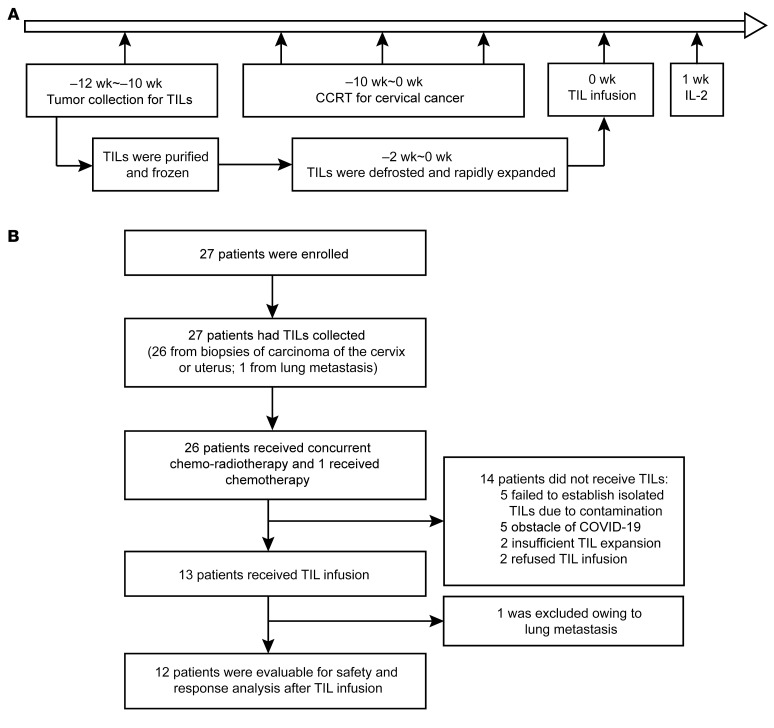
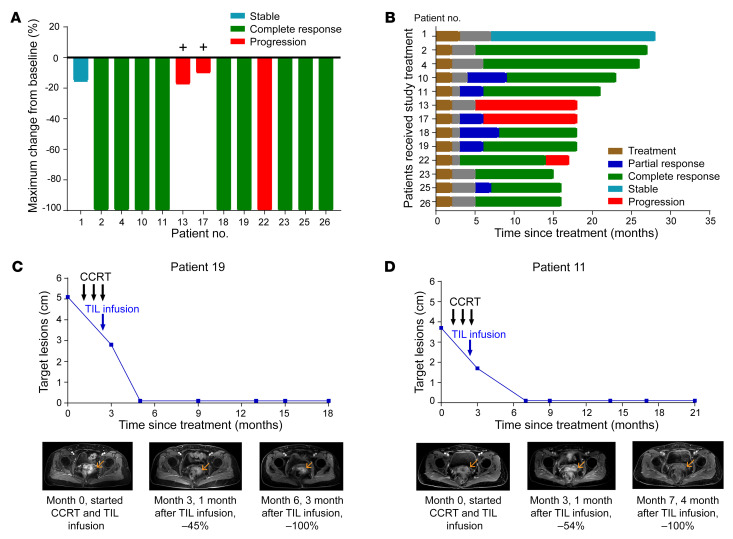
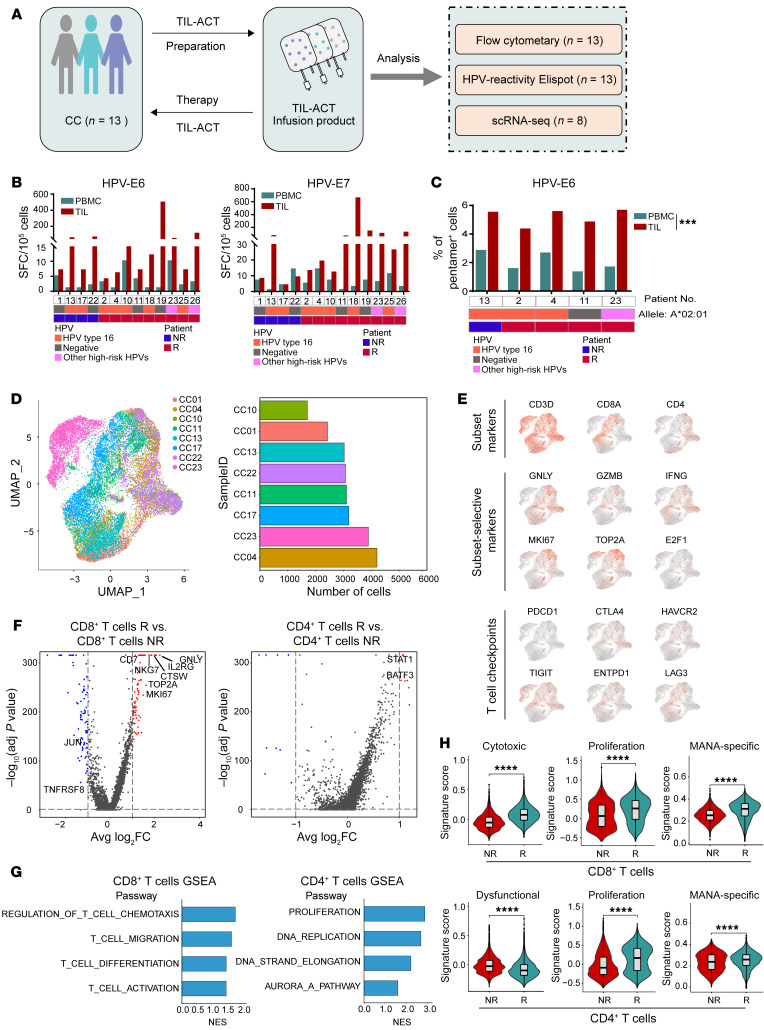
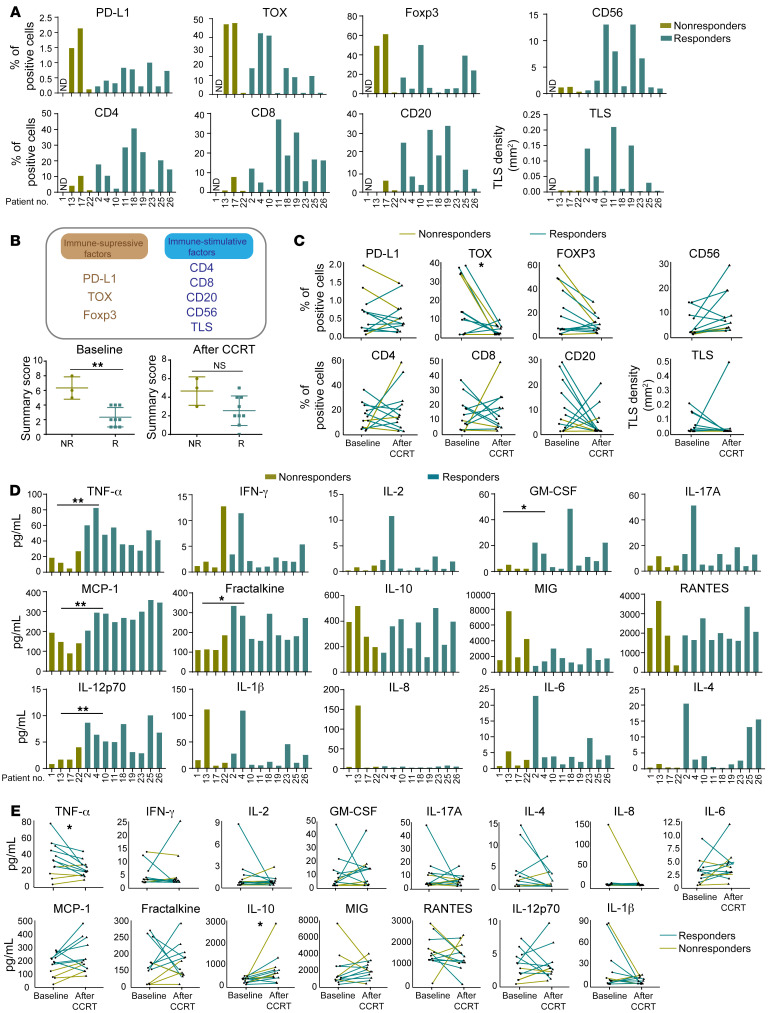
BACKGROUNDAdoptive cell therapy (ACT) with tumor-infiltrating lymphocytes (TILs) has achieved remarkable clinical efficacy in metastatic cancers such as melanoma and cervical cancer (CC). Here, we explored the safety, feasibility, and preliminary tumor response and performed translational investigations of adjuvant immunotherapy using infusion of autogenous TILs (auto-TILs) following concurrent chemoradiotherapy (CCRT) in patients with CC who had locally advanced disease.METHODSTwenty-seven patients with CC with stage III-IV disease were recruited in this single-center, phase I study. TILs were isolated from lesions in the uterine cervix and generated under good manufacturing practice (GMP) conditions and then infused after CCRT plus i.m. IL-2 injections.RESULTSTILs from 20 of the 27 patients were successfully expanded, with a feasibility of 74.1%. Twelve patients received TILs following CCRT. Adverse events (AEs) were primarily attributable to CCRT. Only 1 (8.3%) patient experienced severe toxicity with a grade 3 hypersensitivity reaction after TIL infusion. No autoimmune AEs, such as pneumonitis, hepatitis, or myocarditis, occurred, and there were no treatment-related mortalities. Nine of 12 patients (75.0%) attained a complete response, with a disease control duration of 9-22 months. Translational investigation showed that the transcriptomic characteristics of the infused TIL products and some immune biomarkers in the tumor microenvironment and serum of patients with CC at baseline were correlated with the clinical response.CONCLUSIONTIL-based ACT following CCRT was safe in an academic center setting, with potentially effective responses in patients with locally advanced CC. "Hot" inflammatory immune environments were beneficial to the clinical efficacy of TIL-based ACT as adjuvant therapy.TRIAL REGISTRATIONClinicalTrials.gov NCT04443296.FUNDINGNational Key R&D Program; Sci-Tech Key Program of the Guangzhou City Science Foundation; the Guangdong Province Sci-Tech International Key Program; the National Natural Science Foundation of China.
Keywords: Adaptive immunity; Cancer; Clinical Trials; Oncology.
Figures

References
-
- Chemoradiotherapy for Cervical Cancer Meta-Analysis Collaboration Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: a systematic review and meta-analysis of individual patient data from 18 randomized trials. J Clin Oncol. 2008;26(35):5802–5812. doi: 10.1200/JCO.2008.16.4368. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
