

Antibiotic Prophylaxis to Prevent Obesity-Related Induction Complications in Nulliparae at Term: a pilot randomized controlled trial
- PMID: 35728781
- PMCID: PMC9611553
- DOI: 10.1016/j.ajogmf.2022.100681
Antibiotic Prophylaxis to Prevent Obesity-Related Induction Complications in Nulliparae at Term: a pilot randomized controlled trial
Abstract
Background: Women with obesity are at increased risk of complications during and after labor and delivery, including puerperal infection and cesarean delivery. As labor induction has become increasingly common, it is crucial to find ways to decrease complication rates in this high-risk population.
Objective: This study aimed to explore the effect of prophylactic antibiotics during labor induction of nulliparous women with obesity on the rates of cesarean delivery and puerperal infection and to estimate the parameters needed to calculate the sample size for a larger, multicenter trial.
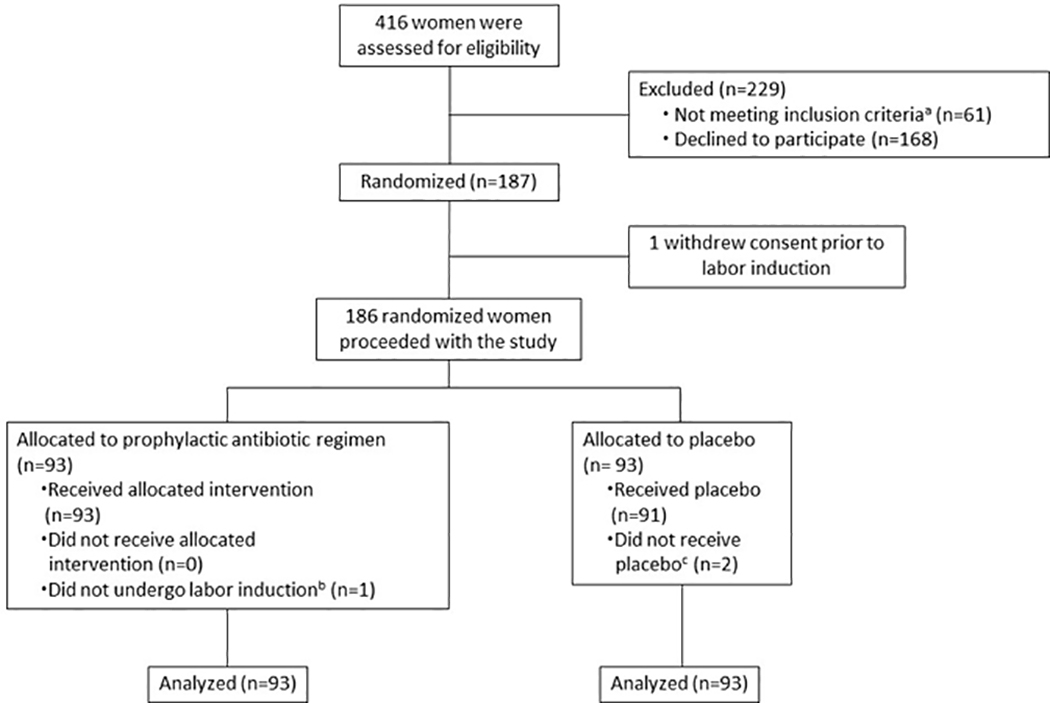
Study design: In this randomized, placebo-controlled pilot trial, nulliparous patients with a body mass index of ≥30 kg/m2 were randomized to either prophylactic antibiotics (500 mg azithromycin for 1 dose and 2 g cefazolin every 8 hours for up to 3 doses) or placebo, administered starting at the beginning of labor induction. The exclusion criteria were known fetal anomaly, fetal demise, multifetal gestation, ruptured membranes >12 hours, infection requiring antibiotics at the start of labor induction, and/or allergy to azithromycin or beta-lactam antibiotics. The co-primary outcomes were rates of puerperal infection (composite of chorioamnionitis, endometritis, and/or cesarean delivery wound infection) and cesarean delivery. Participants were followed up for 30 days after delivery, and maternal and neonatal demographic and outcome data were collected. Proportions and 95% confidence limits were calculated for each of these outcomes.
Results: From January 2019 to May 2021, 101 patients were randomized in the class III stratum (1 patient who was randomized ultimately did not undergo labor induction). From February 2020 to May 2021, 38 and 47 patients were randomized to class I and II strata, respectively (to assess the effect of obesity class on the outcomes expected to be influenced by antibiotic prophylaxis). In the antibiotics and placebo groups, the rates of cesarean delivery were 29.0% (95% confidence interval, 19.8-38.3) and 39.8% (95% confidence interval, 29.8-49.7), respectively, and puerperal infection occurred in 8.6% (95% confidence interval, 2.9-14.3) and 9.7% (95% confidence interval, 3.7-15.7), respectively. In the subgroup with class III obesity, in the antibiotics and placebo groups, the rates of cesarean delivery were 33.3% (95% confidence interval, 20.4-47.9) and 46.0% (95% confidence interval, 32.2-59.8), respectively, and puerperal infection occurred in 7.8% (95% confidence interval, 0.5-15.2) and 10.0% (95% confidence interval, 1.7-18.3), respectively. Note that this pilot study was not powered to detect differences of this magnitude but rather to estimate parameters.
Conclusion: The administration of prophylactic antibiotics during labor induction of nulliparous patients with obesity resulted in a 27% lower cesarean delivery rate overall and a 28% lower rate in patients with class III obesity. A larger trial is warranted to evaluate these differences.
Trial registration: ClinicalTrials.gov NCT03801252.
Keywords: cesarean; cesarean delivery rate; chorioamnionitis; endometritis; labor induction; obese; obesity; pilot study; puerperal infection; wound infection.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Driscoll AK, Gregory ECW. Increases in prepregnancy obesity: United States, 2016–2019. NCHS Data Brief, no 392. Hyattsville, MD: National Center for Health Statistics. 2020. - PubMed
-
- Sibai BM, Ewell M, Levine RJ, et al. Risk factors associated with preeclampsia in healthy nulliparous women. The Calcium for Preeclampsia Prevention (CPEP) Study Group. Am J Obstet Gynecol 1997; 177:1003–10. - PubMed
-
- Weiss JL, Malone FD, Emig D, et al. Obesity, obstetric complications and cesarean delivery rate--a population-based screening study. Am J Obstet Gynecol 2004; 190:1091–7. - PubMed
-
- Nohr EA, Bech BH, Davies MJ, Frydenberg M, Henrikson TB, and Olsen J. Prepregnancy obesity and fetal death: a study within the Danish National Birth Cohort. Obstet Gynecol 2005; 106:250–9. - PubMed
-
- Huang DY, Usher RH, Kramer MS, Yang H, Morin L, and Fretts RC. Determinants of unexplained antepartum fetal deaths. Obstet Gynecol 2000; 95:215–21. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
