

Parallelogram flap versus homodigital island flap in the treatment of fingertip defects with bone exposure: a prospective controlled study
- PMID: 35729610
- PMCID: PMC9210657
- DOI: 10.1186/s13018-022-03214-1
Parallelogram flap versus homodigital island flap in the treatment of fingertip defects with bone exposure: a prospective controlled study
Abstract
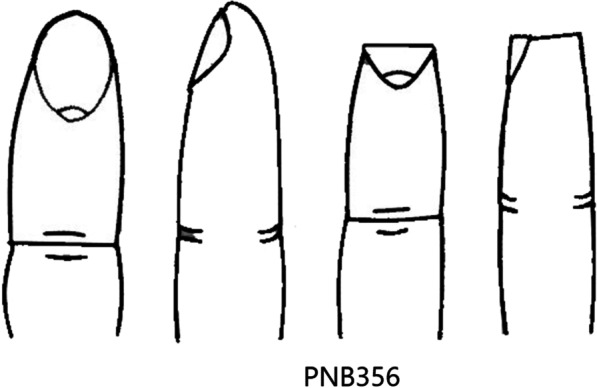
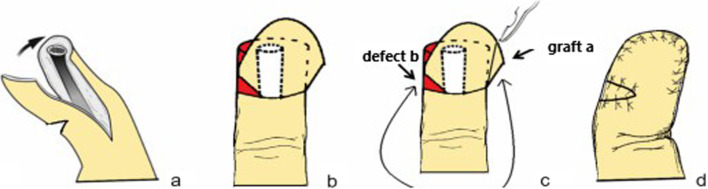
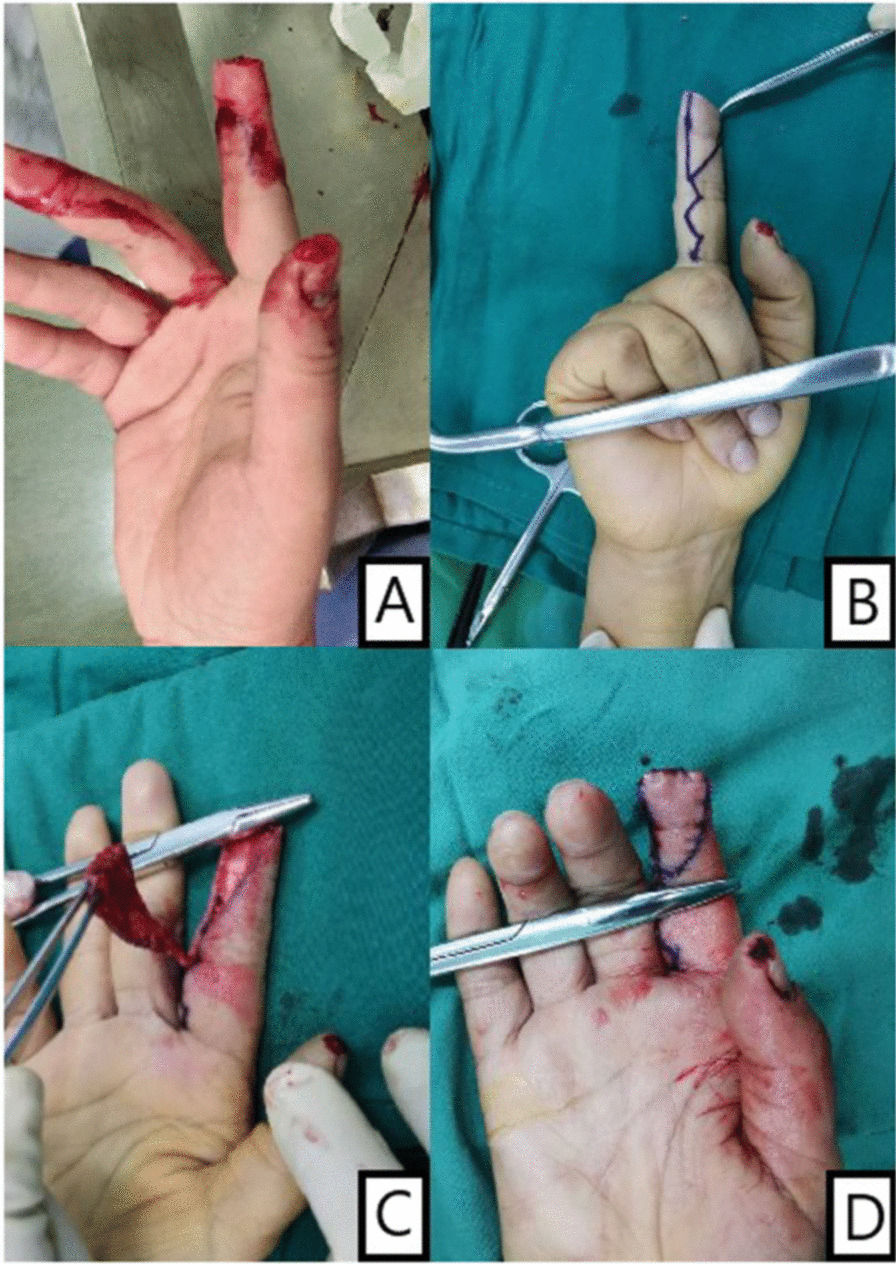
Purpose: A modified local transposition flap (we call it "parallelogram flap") surgery was performed for fingertip injuries. This study aimed to compare the clinical effects of parallelogram flap and homodigital island flaps in fingertip reconstruction.
Methods: The study collected patients who underwent parallelogram transposition flaps and homodigital island flaps to repair fingertip defects from 2019 to 2021. 150 cases (150 fingers) were included in our study. All operations were performed by one surgical team. Record the operation time, two-point discrimination (2PD), Total Active Movement (TAM) and the MHQ (Michigan Hand Questionnaire) of the injured fingers to evaluate the therapeutic effect.
Results: All parallelogram (Group A) and homodigital island flap (Group B) had survived postoperatively. The operative duration of Group A (31.2 ± 3.3 min) is shorter than Group B (97.8 ± 6.1 min) (P < 0.05). At the 6-month follow-up, there was no difference with the two-point discrimination (2PD) of the palmar part of the flaps and the Total Active Movement (TAM) of injured figures in Group A and Group B. The MHQ summary scores in Group A (94.29 ± 3.14) were much higher than in Group B (91.73 ± 3.41) (P < 0.05). Evaluation of the MHQ subscale performance showed that the overall hand function, activities of daily living, work performance and pain score had no differences(P > 0.05), but aesthetics (92.15 ± 7.16) and satisfaction (92.45 ± 5.61) score in Group A was higher than aesthetics (86.56 ± 5.60) and satisfaction (86.72 ± 8.21) score in Group B (P < 0.05 for both).
Conclusions: The reconstruction using parallelogram flaps is a easier and more versatile treatment with better functions, less morbidity and better aesthetics. This method is a better choice for reconstruction of fingertip injury.
Keywords: Bone exposure; Coverage; Defect; Fingertip; Local Flaps; Trauma.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Clinical Application of a Modified Local Transposition Flap (Parallelogram Flap) Surgery in Repairing Fingertip Defects.Ann Plast Surg. 2022 Nov 1;89(5):510-516. doi: 10.1097/SAP.0000000000003283. Ann Plast Surg. 2022. PMID: 36279575 Free PMC article.
-
Comparative Study of the Clinical Effects of Reverse Digital Artery Island Flaps and Antegrade Homodigital Neurovascular Island Flaps for Fingertip Reconstruction.Ann Plast Surg. 2022 Apr 1;88(4):395-400. doi: 10.1097/SAP.0000000000002967. Ann Plast Surg. 2022. PMID: 34334672
-
Reconstruction of multiple fingertip injuries with reverse flow homodigital flap.Injury. 2014 Oct;45(10):1569-73. doi: 10.1016/j.injury.2014.06.009. Epub 2014 Jun 17. Injury. 2014. PMID: 25037528
-
[Homodigital neurovascular island flap according to Venkataswami].Oper Orthop Traumatol. 2020 Dec;32(6):477-485. doi: 10.1007/s00064-020-00681-9. Epub 2020 Nov 13. Oper Orthop Traumatol. 2020. PMID: 33185698 Review. German.
-
Vascularized Heterodigital Island Flap for Fingertip and Dorsal Finger Reconstruction.J Hand Surg Am. 2015 Dec;40(12):2458-64. doi: 10.1016/j.jhsa.2015.06.112. Epub 2015 Aug 29. J Hand Surg Am. 2015. PMID: 26321459 Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
