

A pilot study on the effect of D-allulose on postprandial glucose levels in patients with type 2 diabetes mellitus during Ramadan fasting
- PMID: 35729673
- PMCID: PMC9209837
- DOI: 10.1186/s13098-022-00856-3
A pilot study on the effect of D-allulose on postprandial glucose levels in patients with type 2 diabetes mellitus during Ramadan fasting
Abstract
Background: During Ramadan fasting, postprandial hyperglycemia is commonly observed after iftar (break of fast at sunset) meal. D-allulose is a rare sugar and is reported to have several health benefits, including the suppression of increase in postprandial glucose levels. This study investigates whether D-allulose (a C-3 epimer of D-fructose) improves the postprandial glucose in patients with type 2 diabetes mellitus (T2DM) during Ramadan.
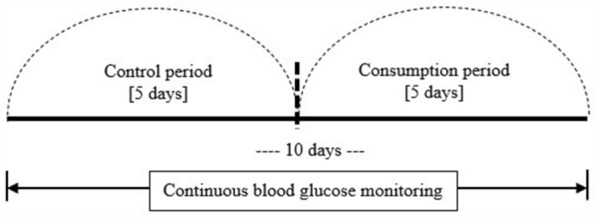
Methods: This was a pilot, prospective single-arm study design that was conducted for 10 consecutive days; 5 days of control and 5 days of consumption. The primary outcome was postprandial peak glucose levels. During the consumption period, 8.5 g of D-allulose was consumed by the participants before iftar meal. Postprandial glucose was measured using a continuous glucose monitoring system.
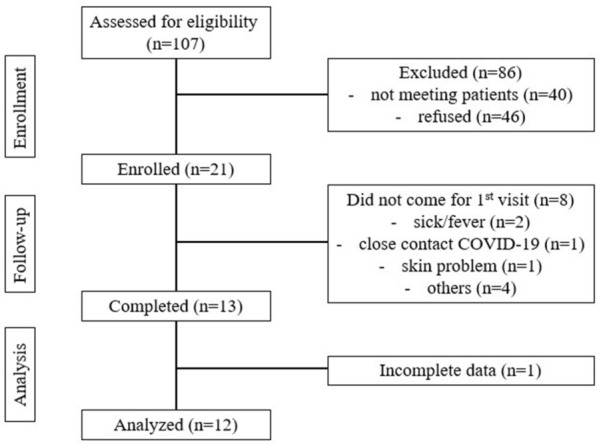
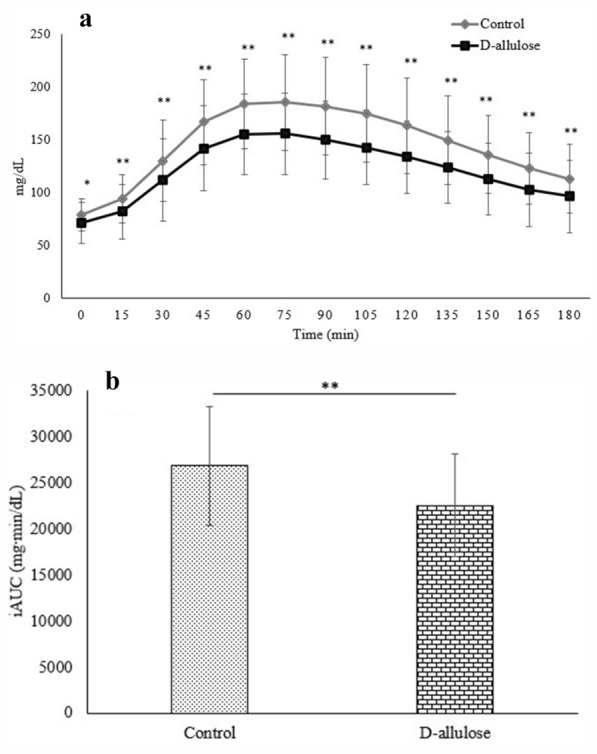
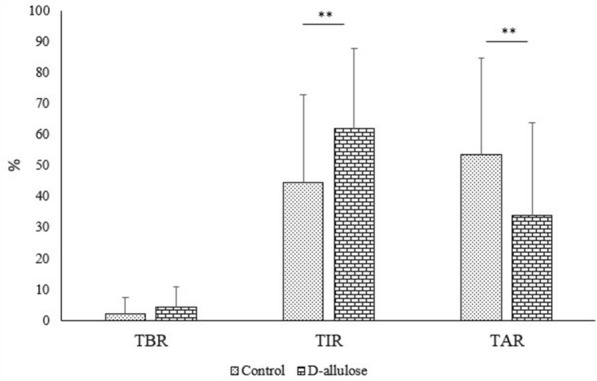
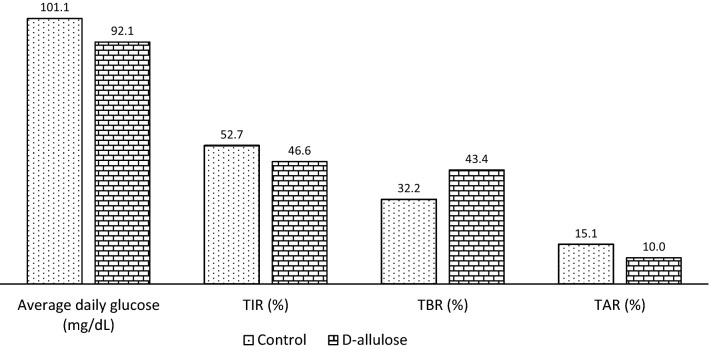
Results: A total of 12 participants completed the study. Significant lower (p < 0.01) postprandial glucose values and the glucose incremental area under the curve (iAUC) were observed from 0 to 180 min during the consumption period compared to the control period. The consumption period demonstrated significantly higher percentages of time in which glucose values were found in the target range (p = 0.0032), and when the glucose levels above the target range were reduced (p = 0.0015).
Conclusions: The supplementation with D-allulose has the potential to improve postprandial hyperglycemia in patients with T2DM after iftar during Ramadan. Further studies are needed to confirm these findings. Trial registration ClinicalTrials.gov NCT05071950. Retrospectively registered, 8 October 2021.
Keywords: CGM; D-allulose; Ramadan; Type 2 diabetes mellitus; postprandial glucose.
© 2022. The Author(s).
Conflict of interest statement
The authors have no competing interest to report.
Figures
References
-
- Jabbar A. Epidemiology of diabetes and Ramadan fasting in diabetes and Ramadan: Practical Guideline. International Diabetes Federation (IDF), in collaboration with the Diabetes and Ramadan (DAR) International Alliance 2016; 17–28.
-
- Ministry of Health Malaysia. National health and morbidity survey 2019: key findings, National Institutes of Health (NIH); 2020.
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
