

Machine learning for improving high-dimensional proxy confounder adjustment in healthcare database studies: An overview of the current literature
- PMID: 35729705
- PMCID: PMC9541861
- DOI: 10.1002/pds.5500
Machine learning for improving high-dimensional proxy confounder adjustment in healthcare database studies: An overview of the current literature
Abstract
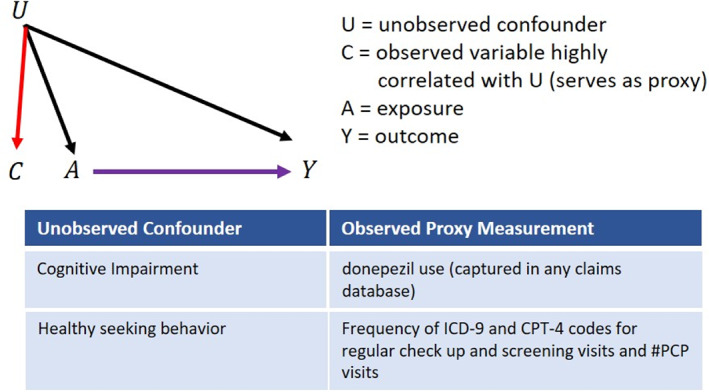
Purpose: Supplementing investigator-specified variables with large numbers of empirically identified features that collectively serve as 'proxies' for unspecified or unmeasured factors can often improve confounding control in studies utilizing administrative healthcare databases. Consequently, there has been a recent focus on the development of data-driven methods for high-dimensional proxy confounder adjustment in pharmacoepidemiologic research. In this paper, we survey current approaches and recent advancements for high-dimensional proxy confounder adjustment in healthcare database studies.
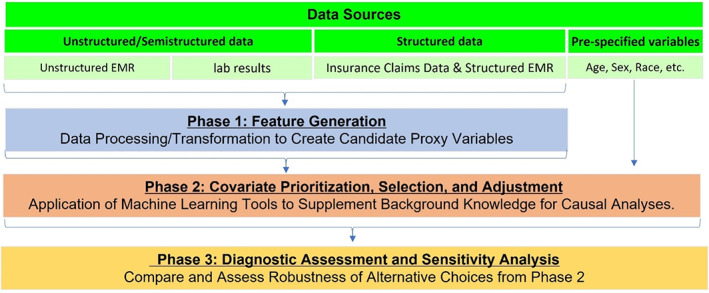
Methods: We discuss considerations underpinning three areas for high-dimensional proxy confounder adjustment: (1) feature generation-transforming raw data into covariates (or features) to be used for proxy adjustment; (2) covariate prioritization, selection, and adjustment; and (3) diagnostic assessment. We discuss challenges and avenues of future development within each area.
Results: There is a large literature on methods for high-dimensional confounder prioritization/selection, but relatively little has been written on best practices for feature generation and diagnostic assessment. Consequently, these areas have particular limitations and challenges.
Conclusions: There is a growing body of evidence showing that machine-learning algorithms for high-dimensional proxy-confounder adjustment can supplement investigator-specified variables to improve confounding control compared to adjustment based on investigator-specified variables alone. However, more research is needed on best practices for feature generation and diagnostic assessment when applying methods for high-dimensional proxy confounder adjustment in pharmacoepidemiologic studies.
Keywords: causal inference; confounding; machine learning.
© 2022 The Authors. Pharmacoepidemiology and Drug Safety published by John Wiley & Sons Ltd.
Conflict of interest statement
Robert W. Platt has consulted for Amgen, Biogen, Merck, Nant Pharma, and Pfizer. Dimitri Bennett is an employee of Takeda. Grammati Sari is employed by Visible Analytics Ltd. Hongbo Yuan is an employee of CADTH. Andrew R. Zullo receives research grant funding from Sanofi Pasteur to support research on infections and vaccinations in nursing homes unrelated to this manuscript. Mugdha Gokhale is a full‐time employee of Merck and owns stocks in Merck. Elisabetta Patorno is supported by a career development grant K08AG055670 from the National Institute on Aging. She is researcher of a researcher‐initiated grant to the Brigham and Women's Hospital from Boehringer Ingelheim, not directly related to the topic of the submitted work.
Figures
References
-
- Corrigan‐Curay J, Sacks L, Woodcock J. Real‐world evidence and real‐world data for evaluating drug safety and effectiveness. JAMA. 2018;320:867‐868. - PubMed
-
- Schneeweiss S, Avorn J. A review of uses of health care utilization databases for epidemiologic research on therapeutics. J Clin Epidemiol. 2005;58:323‐337. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
