

Estrogen Receptor-β Agonists Modulate T-Lymphocyte Activation and Ameliorate Left Ventricular Remodeling During Chronic Heart Failure
- PMID: 35730443
- PMCID: PMC9308745
- DOI: 10.1161/CIRCHEARTFAILURE.121.008997
Estrogen Receptor-β Agonists Modulate T-Lymphocyte Activation and Ameliorate Left Ventricular Remodeling During Chronic Heart Failure
Abstract
Background: CD4+ T cells temporally transition from protective to pathological during ischemic heart failure (HF; 8 weeks postmyocardial infarction). Cellular mechanisms mediating this shift are unknown.
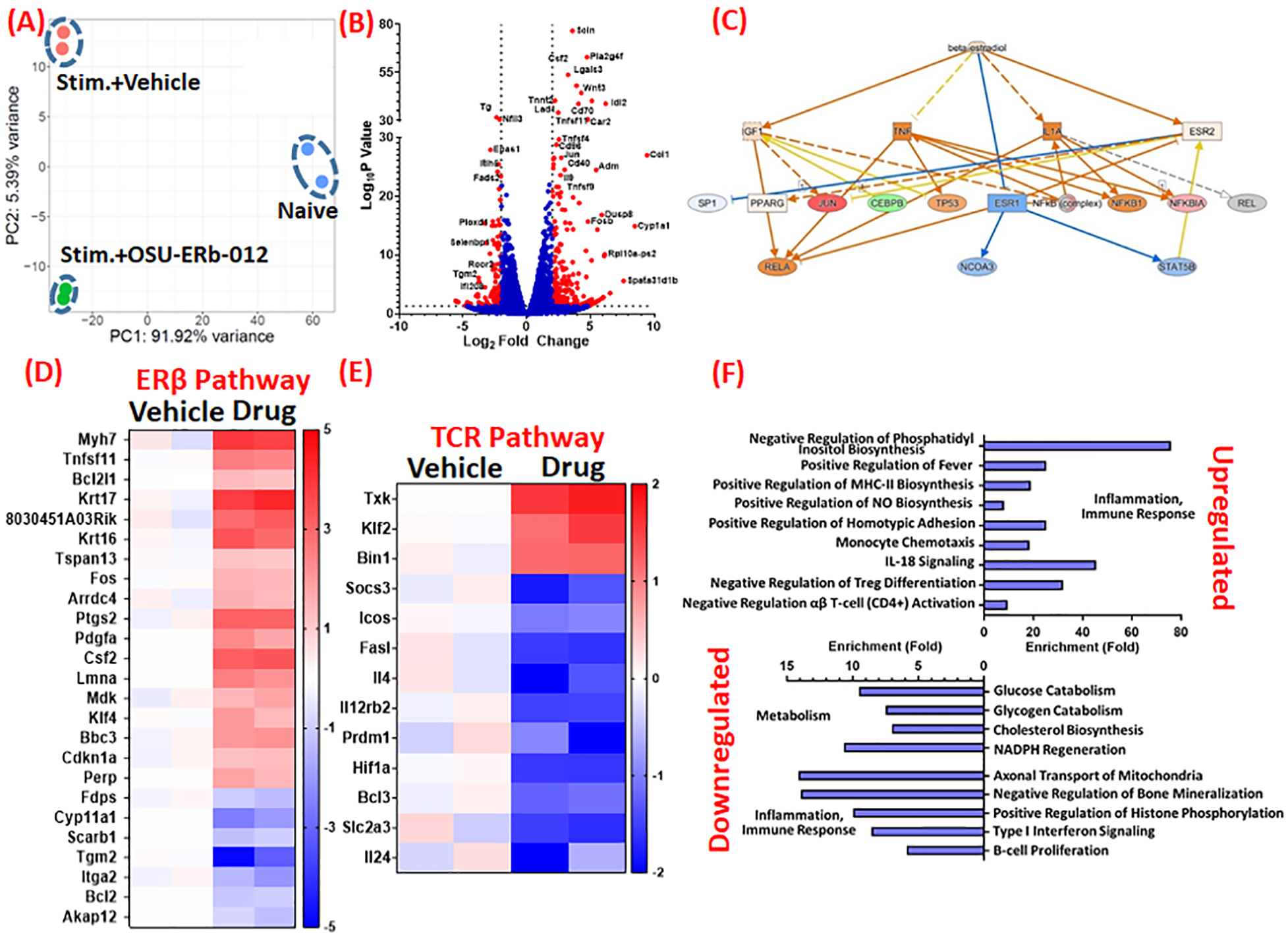
Methods: RNA-sequencing of cardiac CD4+ T cells and flow cytometric analysis of immune cells was conducted.
Results: RNA-sequencing of CD4+ T cells from the failing hearts of male mice indicated activation of ER (estrogen receptor)-α signaling. Flow cytometric analysis showed that ERα in CD4+ T cells decreases significantly at 3-day postmyocardial infarction but increases during HF. To antagonize ERα, we tested a novel ERβ agonist (OSU-ERb-012) to inhibit T cells and blunt left ventricular remodeling. Proliferation assays showed that OSU-ERb-012 dose-dependently inhibited proliferation and proinflammatory cytokine expression in anti-CD3/CD28 stimulated splenic T cells isolated from both the sexes. For in vivo efficacy, 10- to 12-week-old male and ovariectomized female mice were randomized at 4 weeks postmyocardial infarction and treated with either vehicle or drug (60 mg/kg per day; oral). While vehicle-treated HF mice displayed progressive left ventricular dilatation with significantly increased end-systolic and end-diastolic volumes from 4 to 8 weeks postmyocardial infarction, treatment with OSU-ERb-012 significantly blunted these changes and stopped left ventricular remodeling in both the sexes. Reduction in tibia-normalized heart and left ventricular weights, cardiomyocyte hypertrophy and interstitial fibrosis further supported these results. Additionally, OSU-ERb-012 treatment selectively inhibited cardiac, splenic, and circulating CD4+ T cells without affecting other myeloid and lymphoid cells in the HF mice.
Conclusions: Our studies indicate that ERβ agonists and OSU-ERb-012, in particular, could be used as selective immunomodulatory drugs to inhibit CD4+ T cells during chronic HF.
Keywords: T-lymphocytes; heart failure; myocardial infarction; receptor, estrogen; ventricular remodeling.
Conflict of interest statement
Figures





References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
