

Rheumatic Heart Disease Is a Neglected Disease Relative to Its Burden Worldwide: Findings From Global Burden of Disease 2019
- PMID: 35730651
- PMCID: PMC9333364
- DOI: 10.1161/JAHA.122.025284
Rheumatic Heart Disease Is a Neglected Disease Relative to Its Burden Worldwide: Findings From Global Burden of Disease 2019
Abstract
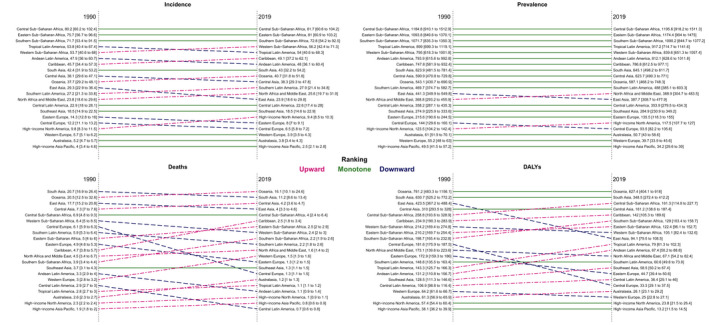
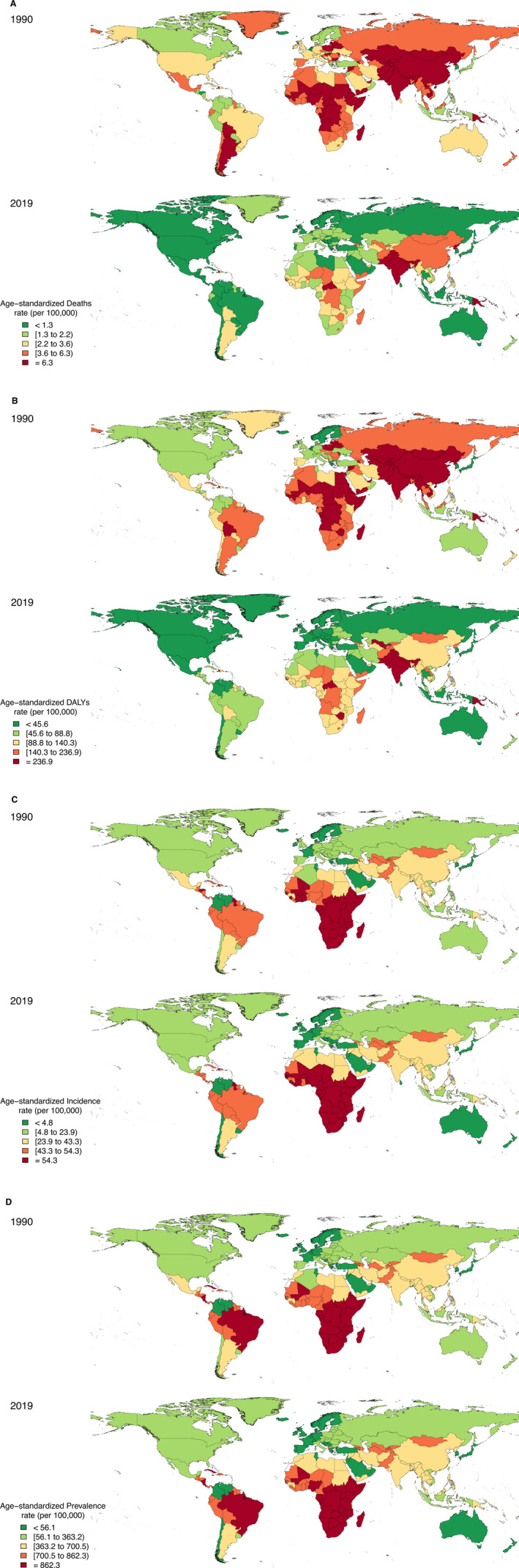
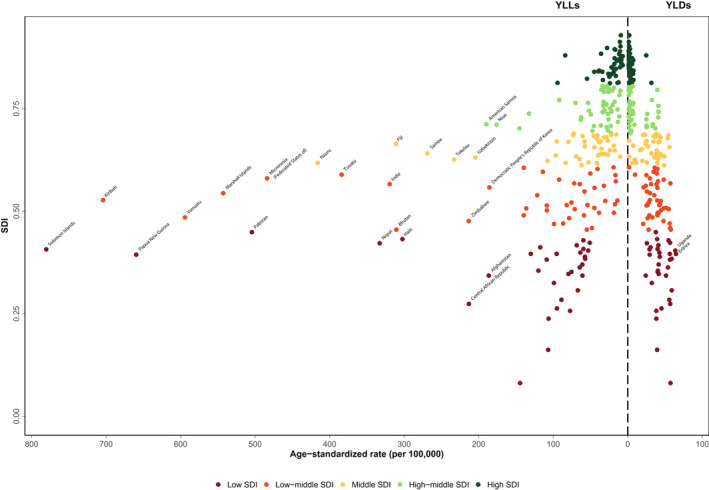
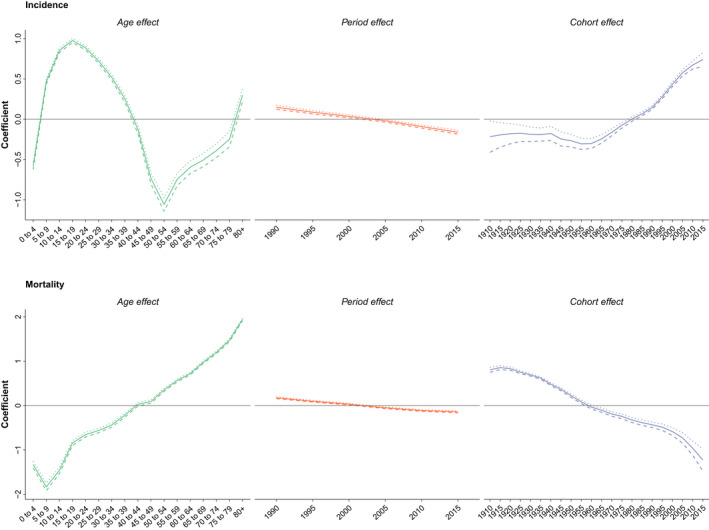
Background Rheumatic heart disease (RHD) takes a heavy toll in low- and middle-income countries. We aimed to present worldwide estimates for the burden of the RHD during 1990 to 2019 using the GBD (Global Burden of Disease) study. Methods and Results Sociodemographic index (SDI) and age-period-cohort analysis were used to assess inequity. The age-standardized death, disability-adjusted life years, incidence, and prevalence rates of RHD were 3.9 (95% uncertainty interval, 3.3-4.3), 132.9 (95% uncertainty interval, 115.0-150.3), 37.4 (28.6-46.7), and 513.7 (405.0-636.3) per 100 000 in 2019, respectively. The age-standardized incidence and prevalence rates increased by 14.4% and 13.8%, respectively. However, disability-adjusted life years and death rates decreased by 53.1% and 56.9%, respectively. South Asia superregion had the highest age-standardized disability-adjusted life years and deaths. Sub-Saharan Africa had the highest age-standardized incidence and prevalence rates. There was a steep decline in RHD burden among higher-SDI countries. However, only age-standardized deaths and disability-adjusted life years rates decreased in lower-SDI countries. The age-standardized years of life lost and years lived with disability rates for RHD significantly declined as countries' SDI increased. The coefficients of birth cohort effect on the incidence of RHD showed an increasing trend from 1960 to 1964 to 2015 to 2019; however, the birth cohort effect on deaths attributable to RHD showed unfailingly decreasing trends from 1910 to 1914 to 2015 to 2019. Conclusions There was a divergence in the burden of RHD among countries based on SDI levels, which calls for including RHD in global assistance and funding. Indeed, many countries are still dealing with an unfinished infectious disease agenda, and there is an urgency to act now to prevent an increase in future RHD burden.
Keywords: disability‐adjusted life years; global burden of disease; heart; rheumatic fever; rheumatic heart disease.
Figures

References
-
- Bennett J, Zhang J, Leung W, Jack S, Oliver J, Webb R, Wilson N, Sika‐Paotonu D, Harwood M, Baker MG. Rising ethnic inequalities in acute rheumatic fever and rheumatic heart disease, New Zealand, 2000–2018—Volume 27, Number 1—January 2021—emerging infectious diseases journal—CDC. Emerg Infect Dis. 2021;27:36–46. - PMC - PubMed
-
- Kang K, Chau K, Howell E, Anderson M, Smith S, Davis TJ, Starmer G, Hanson J. The temporospatial epidemiology of rheumatic heart disease in Far North Queensland, tropical Australia 1997–2017; impact of socioeconomic status on disease burden, severity and access to care. PLoS Negl Trop Dis. 2021;15:1–20. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
