

Limitations of Molecular and Antigen Test Performance for SARS-CoV-2 in Symptomatic and Asymptomatic COVID-19 Contacts
- PMID: 35730949
- PMCID: PMC9297839
- DOI: 10.1128/jcm.00187-22
Limitations of Molecular and Antigen Test Performance for SARS-CoV-2 in Symptomatic and Asymptomatic COVID-19 Contacts
Abstract
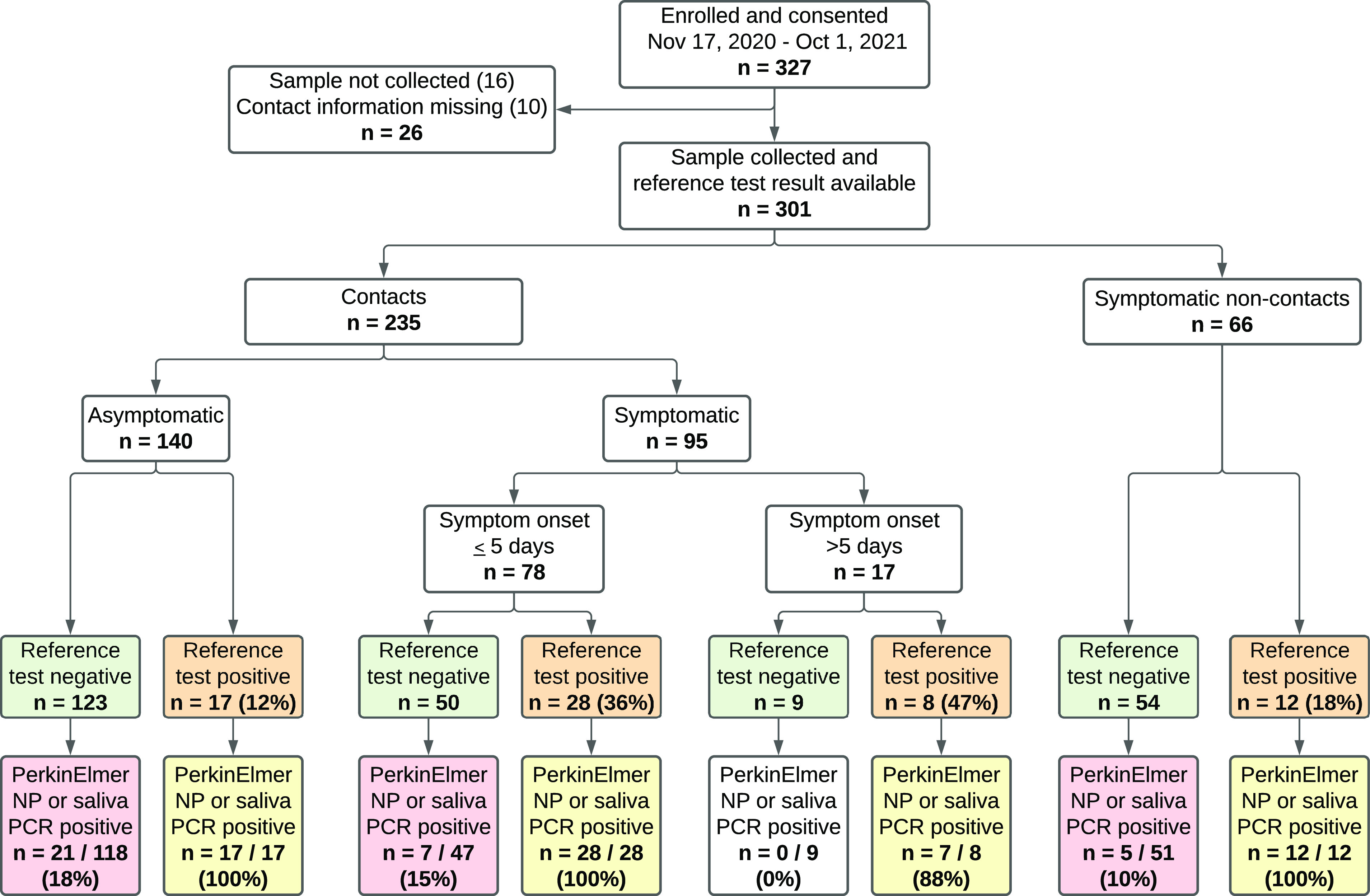
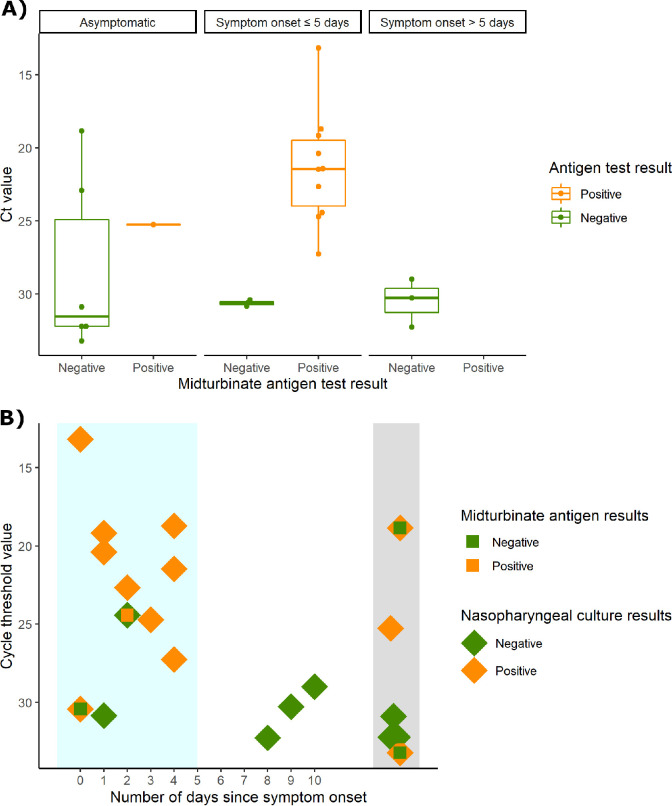
COVID-19 has brought unprecedented attention to the crucial role of diagnostics in pandemic control. We compared severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) test performance by sample type and modality in close contacts of SARS-CoV-2 cases. Close contacts of SARS-CoV-2-positive individuals were enrolled after informed consent. Clinician-collected nasopharyngeal (NP) swabs in viral transport media (VTM) were tested with a routine clinical reference nucleic acid test (NAT) and PerkinElmer real-time reverse transcription-PCR (RT-PCR) assay; positive samples were tested for infectivity using a VeroE6TMPRSS2 cell culture model. Self-collected passive drool was also tested using the PerkinElmer RT-PCR assay. For the first 4 months of study, midturbinate swabs were tested using the BD Veritor rapid antigen test. Between 17 November 2020 and 1 October 2021, 235 close contacts of SARS-CoV-2 cases were recruited, including 95 with symptoms (82% symptomatic for ≤5 days) and 140 asymptomatic individuals. Reference NATs were positive for 53 (22.6%) participants; 24/50 (48%) were culture positive. PerkinElmer testing of NP and saliva samples identified an additional 28 (11.9%) SARS-CoV-2 cases who tested negative by reference NAT. Antigen tests performed for 99 close contacts showed 83% positive percent agreement (PPA) with reference NAT among early symptomatic persons, but 18% PPA in others; antigen tests in 8 of 11 (72.7%) culture-positive participants were positive. Contacts of SARS-CoV-2 cases may be falsely negative early after contact, but more sensitive platforms may identify these cases. Repeat or serial SARS-CoV-2 testing with both antigen and molecular assays may be warranted for individuals with high pretest probability for infection.
Keywords: COVID-19; SARS-CoV-2; rapid diagnostics; test performance.
Conflict of interest statement
The authors declare a conflict of interest. Becton Dickenson provided Veritor test kits for use in this study but did not contribute to the writing of this manuscript nor critically review its content. D.D.M. reports consulting and research grants from Bristol-Myers Squibb and Pfizer, consulting and research support from Fitbit, consulting and research support from Flexcon, research grant from Boehringer Ingelheim, consulting from Avania, non-financial research support from Apple Computer, consulting/other support from Heart Rhythm Society. L.G.J. is on a scientific advisory board for Moderna on projects unrelated to SARS-CoV-2. H.H.M. reports receipt of research contracts from BioRad, DiaSorin, and Hologic. Y.C.M. has received tests from Quanterix, Becton-Dickinson, Ceres, and Hologic for research-related purposes, consults for Abbott on subjects unrelated to SARS-CoV-2, and receives funding support to Johns Hopkins University from miDiagnostics.
The authors declare a conflict of interest. Becton Dickenson provided Veritor test kits for use in this study but did not contribute to the writing of this manuscript nor critically review its content. DDM reports consulting and research grants from Bristol-Myers Squibb and Pfizer, consulting and research support from Fitbit, consulting and research support from Flexcon, research grant from Boehringer Ingelheim, consulting from Avania, non-financial research support from Apple Computer, consulting/other support from Heart Rhythm Society. LG is on a scientific advisory board for Moderna on projects unrelated to SARS-CoV-2. HHM reports receipt of research contracts from BioRad, DiaSorin, and Hologic. YCM has received tests from Quanterix, Becton-Dickinson, Ceres, and Hologic for research-related purposes, consults for Abbott on subjects unrelated to SARS-CoV-2, and receives funding support to Johns Hopkins University from miDiagnostics.
Figures
Update of
-
Limitations of molecular and antigen test performance for SARS-CoV-2 in symptomatic and asymptomatic COVID-19 contacts.medRxiv [Preprint]. 2022 Feb 7:2022.02.05.22270481. doi: 10.1101/2022.02.05.22270481. medRxiv. 2022. Update in: J Clin Microbiol. 2022 Jul 20;60(7):e0018722. doi: 10.1128/jcm.00187-22. PMID: 35169814 Free PMC article. Updated. Preprint.
References
-
- Mackay MJ, Hooker AC, Afshinnekoo E, Salit M, Kelly J, Feldstein JV, Haft N, Schenkel D, Nambi S, Cai Y, Zhang F, Church G, Dai J, Wang CL, Levy S, Huber J, Ji HP, Kriegel A, Wyllie AL, Mason CE. 2020. The COVID-19 XPRIZE and the need for scalable, fast, and widespread testing. Nat Biotechnol 38:1021–1024. 10.1038/s41587-020-0655-4. - DOI - PMC - PubMed
-
- U.S. Food and Drug Administration. 2020. Coronavirus (COVID-19) update: FDA publishes comparative performance data for COVID-19 molecular diagnostic tests. U.S. Food and Drug Administration, Washington, DC. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19....
-
- Dinnes J, Deeks JJ, Adriano A, Berhane S, Davenport C, Dittrich S, Emperador D, Takwoingi Y, Cunningham J, Beese S, Dretzke J, Ferrante di Ruffano L, Harris IM, Price MJ, Taylor-Phillips S, Hooft L, Leeflang MM, Spijker R, Van den Bruel A, Cochrane COVID-19 Diagnostic Test Accuracy Group. 2020. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst Rev 8:CD013705. 10.1002/14651858.CD013705. - DOI - PMC - PubMed
-
- Centers for Disease Control and Prevention. 2021. Appendix A – glossary of key terms, close contact. Centers for Disease Control and Prevention, Atlanta, GA. https://www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tr.... Accessed 15 July 2021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
