

Right temporal degeneration and socioemotional semantics: semantic behavioural variant frontotemporal dementia
- PMID: 35731122
- PMCID: PMC10200288
- DOI: 10.1093/brain/awac217
Right temporal degeneration and socioemotional semantics: semantic behavioural variant frontotemporal dementia
Abstract
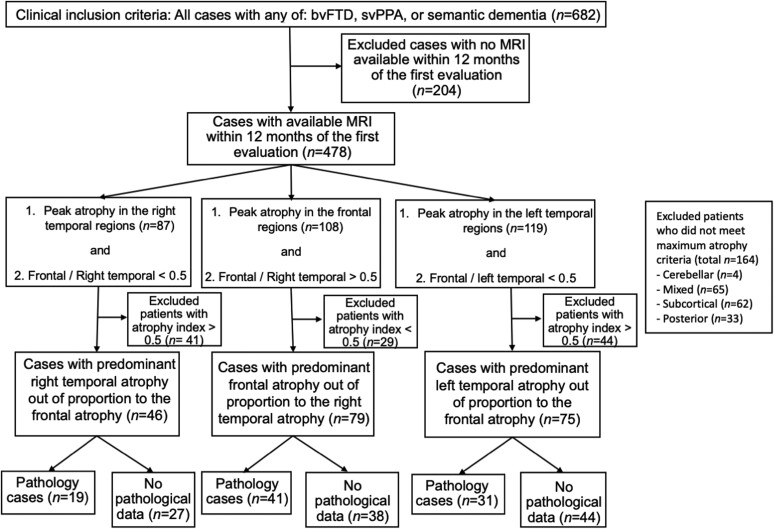
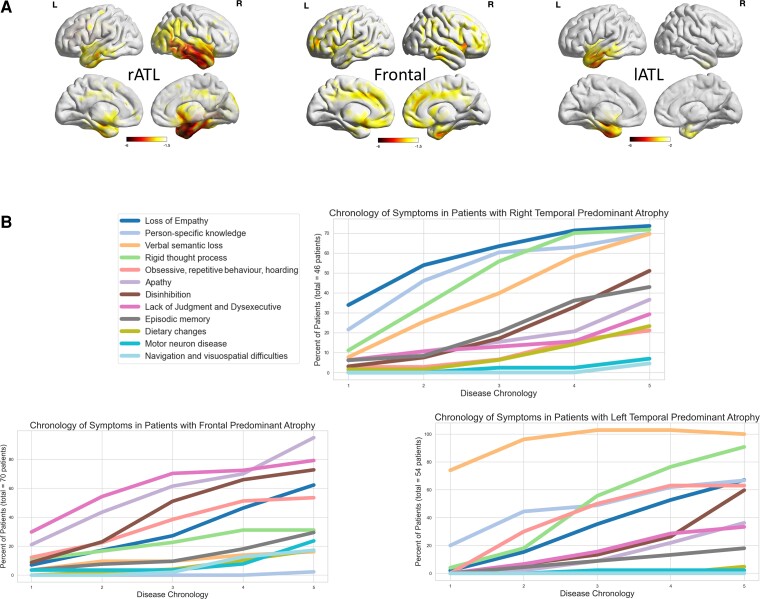
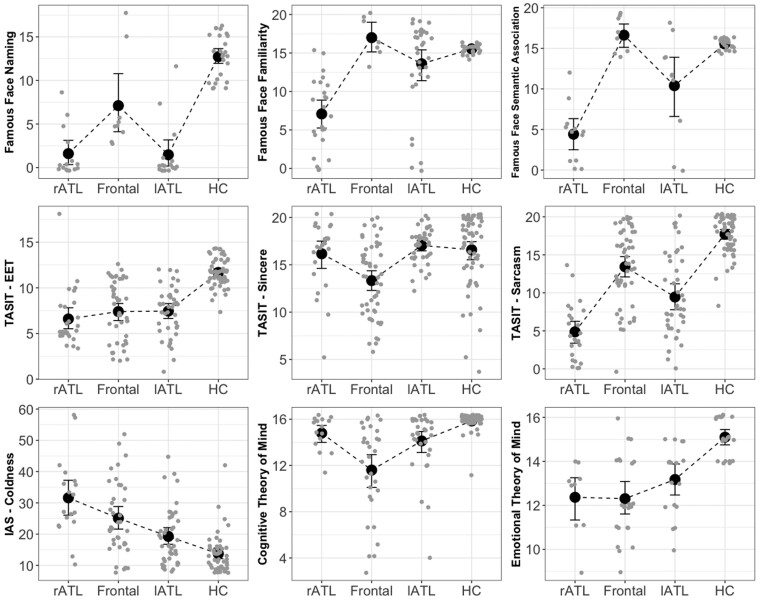
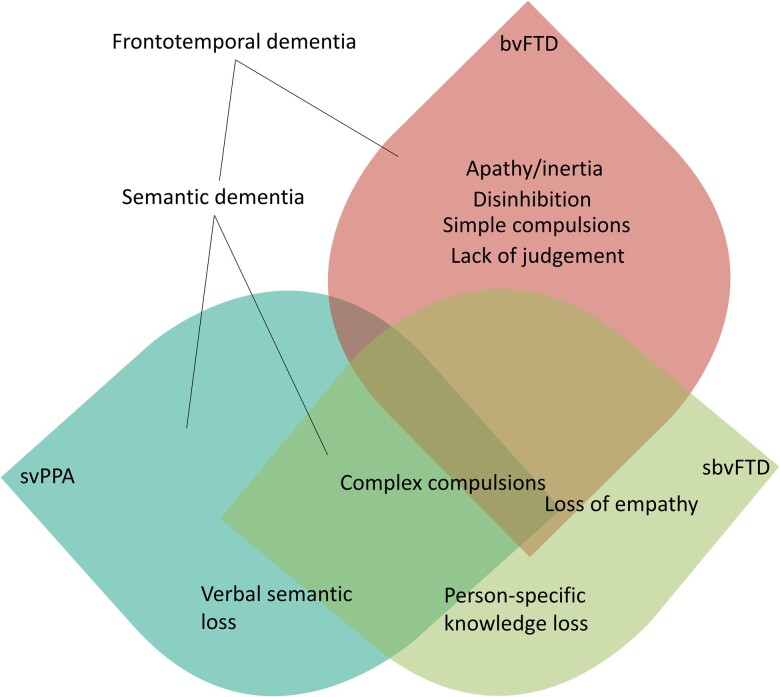
Focal anterior temporal lobe degeneration often preferentially affects the left or right hemisphere. While patients with left-predominant anterior temporal lobe atrophy show severe anomia and verbal semantic deficits and meet criteria for semantic variant primary progressive aphasia and semantic dementia, patients with early right anterior temporal lobe atrophy are more difficult to diagnose as their symptoms are less well understood. Focal right anterior temporal lobe atrophy is associated with prominent emotional and behavioural changes, and patients often meet, or go on to meet, criteria for behavioural variant frontotemporal dementia. Uncertainty around early symptoms and absence of an overarching clinico-anatomical framework continue to hinder proper diagnosis and care of patients with right anterior temporal lobe disease. Here, we examine a large, well-characterized, longitudinal cohort of patients with right anterior temporal lobe-predominant degeneration and propose new criteria and nosology. We identified individuals from our database with a clinical diagnosis of behavioural variant frontotemporal dementia or semantic variant primary progressive aphasia and a structural MRI (n = 478). On the basis of neuroimaging criteria, we defined three patient groups: right anterior temporal lobe-predominant atrophy with relative sparing of the frontal lobes (n = 46), frontal-predominant atrophy with relative sparing of the right anterior temporal lobe (n = 79) and left-predominant anterior temporal lobe-predominant atrophy with relative sparing of the frontal lobes (n = 75). We compared the clinical, neuropsychological, genetic and pathological profiles of these groups. In the right anterior temporal lobe-predominant group, the earliest symptoms were loss of empathy (27%), person-specific semantic impairment (23%) and complex compulsions and rigid thought process (18%). On testing, this group exhibited greater impairments in Emotional Theory of Mind, recognition of famous people (from names and faces) and facial affect naming (despite preserved face perception) than the frontal- and left-predominant anterior temporal lobe-predominant groups. The clinical symptoms in the first 3 years of the disease alone were highly sensitive (81%) and specific (84%) differentiating right anterior temporal lobe-predominant from frontal-predominant groups. Frontotemporal lobar degeneration-transactive response DNA binding protein (84%) was the most common pathology of the right anterior temporal lobe-predominant group. Right anterior temporal lobe-predominant degeneration is characterized by early loss of empathy and person-specific knowledge, deficits that are caused by progressive decline in semantic memory for concepts of socioemotional relevance. Guided by our results, we outline new diagnostic criteria and propose the name, 'semantic behavioural variant frontotemporal dementia', which highlights the underlying cognitive mechanism and the predominant symptomatology. These diagnostic criteria will facilitate early identification and care of patients with early, focal right anterior temporal lobe degeneration as well as in vivo prediction of frontotemporal lobar degeneration-transactive response DNA binding protein pathology.
Keywords: FTLD-TDP type C; frontotemporal dementia; loss of empathy and non-verbal semantics; person-specific knowledge; right temporal lobe-predominant neurodegeneration.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Miller BL, Chang L, Mena I, Boone K, Lesser IM. Progressive right frontotemporal degeneration: Clinical, neuropsychological and SPECT characteristics. Dementia. 1993;4:204–213. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P50 AG023501/AG/NIA NIH HHS/United States
- K24 AG045333/AG/NIA NIH HHS/United States
- RF1 AG029577/AG/NIA NIH HHS/United States
- K24 AG053435/AG/NIA NIH HHS/United States
- R01 AG029577/AG/NIA NIH HHS/United States
- R01 AG052496/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- K08 AG052648/AG/NIA NIH HHS/United States
- R01 NS050915/NS/NINDS NIH HHS/United States
- K24 DC015544/DC/NIDCD NIH HHS/United States
- R01 AG059794/AG/NIA NIH HHS/United States
- R01 AG038791/AG/NIA NIH HHS/United States
- U54 NS092089/NS/NINDS NIH HHS/United States
- R01 AG062758/AG/NIA NIH HHS/United States
- RF1 NS050915/NS/NINDS NIH HHS/United States
