

Health-related quality of life following FDG-PET/CT for cytological indeterminate thyroid nodules
- PMID: 35731242
- PMCID: PMC9346328
- DOI: 10.1530/EC-22-0014
Health-related quality of life following FDG-PET/CT for cytological indeterminate thyroid nodules
Abstract
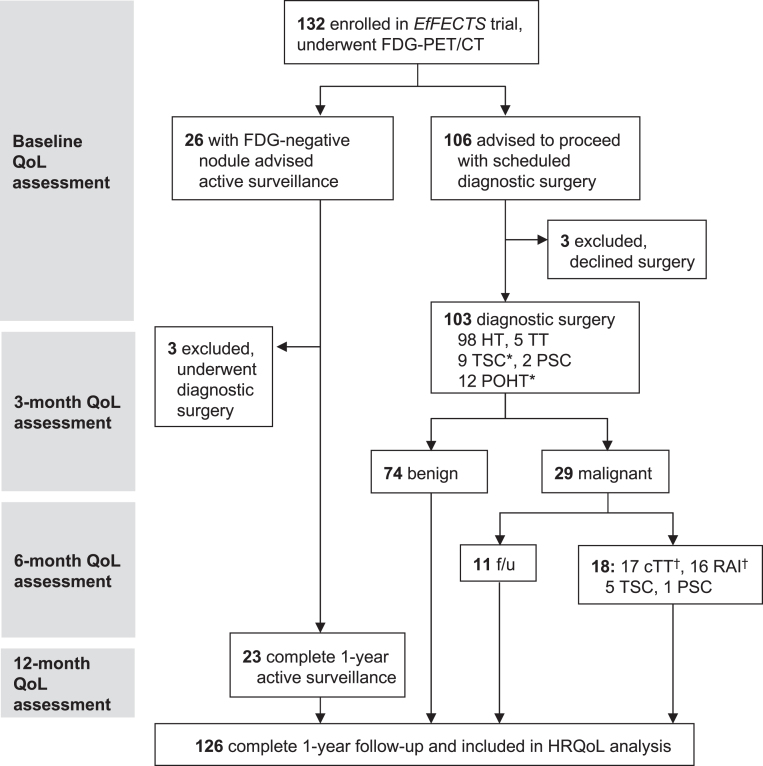
Objective: This study assessed the health-related quality of life (HRQoL) in patients undergoing 2-[18F]fluoro-2-deoxy-D-glucose (FDG)-PET/CT for an indeterminate (Bethesda III/IV) thyroid nodule. FDG-PET/CT accurately rules out malignancy and prevents 40% of futile diagnostic surgeries in these nodules.
Design: Secondary analyses of HRQoL data from a randomised controlled multicentre trial (NCT02208544) in 126 patients from 15 hospitals in the Netherlands were done.
Methods: Longitudinal HRQoL assessment was performed using the EuroQol 5-dimension 5-level (EQ-5D-5L), the RAND 36-item Health Survey v2.0 (RAND-36), and the Thyroid Patient-Reported Outcome (ThyPRO) questionnaire on baseline, 3, 6, and 12 months, relative to the date of the FDG-PET/CT scan.
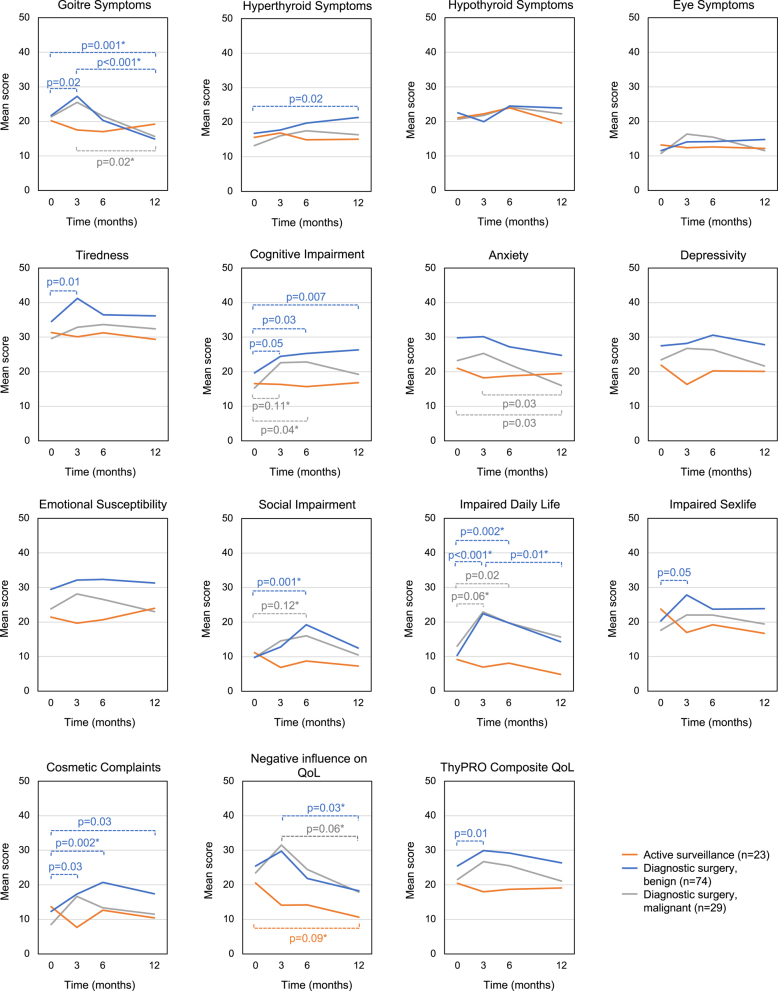
Results: Patients who were randomised to active surveillance following an FDG-negative nodule instead of diagnostic surgery reported stable HRQoL scores throughout the year. Univariate analysis indicated better HRQoL for patients undergoing surveillance than surgical patients with benign histopathology on multiple physical and psychosocial domains. Univariate within-group analysis suggested both temporary and continued HRQoL deteriorations in patients with benign histopathology over time. Multivariate within-group analysis demonstrated no significant longitudinal HRQoL changes in patients undergoing active surveillance. In contrast, in patients with benign histopathology, worse HRQoL was observed with regard to ThyPRO cognitive impairment (P = 0.01) and cosmetic complaints (P = 0.02), whereas goitre symptoms (P < 0.001) and anxiety (P = 0.04) improved over time. In patients with malignant histopathology, anxiety also decreased (P = 0.05).
Conclusions: The reassurance of a negative FDG-PET/CT resulted in sustained HRQoL throughout the first year of active surveillance. Diagnostic surgery for a nodule with benign histopathology resulted in more cognitive impairment and physical problems including cosmetic complaints, but improved goitre symptoms and anxiety. Anxiety was also reduced in patients with malignant histopathology.
Keywords: Bethesda; FDG-PET/CT; diagnostic thyroid surgery; health-related quality of life; indeterminate cytology; thyroid nodule.
Figures
References
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, et al.2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016261–133. (10.1089/thy.2015.0020) - DOI - PMC - PubMed
-
- de Koster EJ, de Geus-Oei LF, Dekkers OM, van Engen-van Grunsven I, Hamming J, Corssmit EPM, Morreau H, Schepers A, Smit J, Oyen WJG, et al.Diagnostic utility of molecular and imaging biomarkers in cytological indeterminate thyroid nodules. Endocrine Reviews 201839154–191. (10.1210/er.2017-00133) - DOI - PubMed
LinkOut - more resources
Full Text Sources
