

Cost-effectiveness of Pulmonary Rehabilitation Among US Adults With Chronic Obstructive Pulmonary Disease
- PMID: 35731514
- PMCID: PMC9218844
- DOI: 10.1001/jamanetworkopen.2022.18189
Cost-effectiveness of Pulmonary Rehabilitation Among US Adults With Chronic Obstructive Pulmonary Disease
Erratum in
-
Error in Table.JAMA Netw Open. 2022 Jul 1;5(7):e2225391. doi: 10.1001/jamanetworkopen.2022.25391. JAMA Netw Open. 2022. PMID: 35834259 Free PMC article. No abstract available.
Abstract
Importance: Pulmonary rehabilitation (PR) after exacerbation of chronic obstructive pulmonary disease (COPD) is effective in reducing COPD hospitalizations and mortality while improving health-related quality of life, yet use of PR remains low. Estimates of the cost-effectiveness of PR in this setting could inform policies to improve uptake.
Objective: To estimate the cost-effectiveness of participation in PR after hospitalization for COPD.
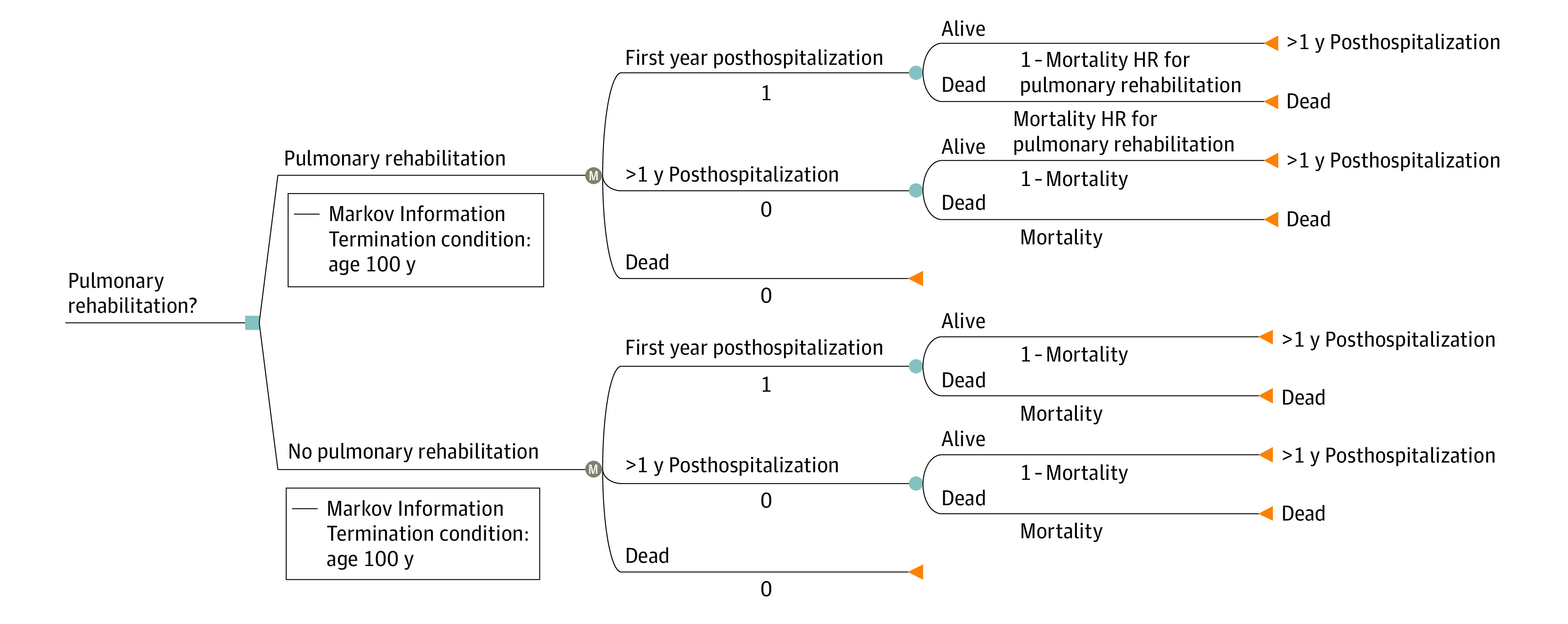
Design, setting, and participants: This economic evaluation estimated the cost-effectiveness of participation in PR compared with no PR after COPD hospitalization in the US using a societal perspective analysis. A Markov microsimulation model was developed to estimate the cost-effectiveness in the US health care system with a lifetime horizon, 1-year cycle length, and a discounted rate of 3% per year for both costs and outcomes. Data sources included published literature from October 1, 2001, to April 1, 2021, with the primary source being an analysis of Medicare beneficiaries living with COPD between January 1, 2014, and December 31, 2015. The analysis was designed and conducted from October 1, 2019, to December 15, 2021. A base case microsimulation, univariate analyses, and a probabilistic sensitivity analysis were performed.
Interventions: Pulmonary rehabilitation compared with no PR after COPD hospitalization.
Main outcomes and measures: Net cost in US dollars, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratio.
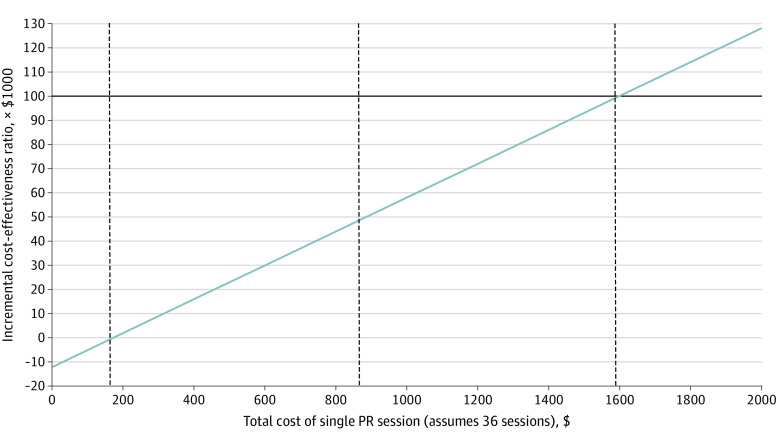
Results: Among the hypothetical cohort with a mean age of 76.9 (age range, 60-92) years and 58.6% women, the base case microsimulation from a societal perspective demonstrated that PR resulted in net cost savings per patient of $5721 (95% prediction interval, $3307-$8388) and improved quality-adjusted life expectancy (QALE) (gain of 0.53 [95% prediction interval, 0.43-0.63] years). The findings of net cost savings and improved QALE with PR did not change in univariate analyses of patient age, the Global Initiative for Obstructive Lung Disease stage, or number of PR sessions. In a probabilistic sensitivity analysis, PR resulted in net cost savings and improved QALE in every one of 1000 samples and was the dominant strategy in 100% of simulations at any willingness-to-pay threshold. In a 1-way sensitivity analysis of total cost, assuming completion of 36 sessions, a single PR session would remain cost saving to $171 per session and had an incremental cost-effectiveness ratio of $884 per session for $50 000/QALY and $1597 per session for $100 000/QALY.
Conclusions and relevance: In this economic evaluation, PR after COPD hospitalization appeared to result in net cost savings along with improvement in QALE. These findings suggest that stakeholders should identify policies to increase access and adherence to PR for patients with COPD.
Conflict of interest statement
Figures
References
-
- Mannino DM, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance--United States, 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16. - PubMed
-
- National Center for Health Statistics . Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. National Center for Health Statistics; 2016. - PubMed
-
- Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095-2128. Published correction in Lancet. 2013;381(9867):628. doi: 10.1016/S0140-6736(12)61728-0 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
