

Association of Changes in Antithrombin Activity Over Time With Responsiveness to Enoxaparin Prophylaxis and Risk of Trauma-Related Venous Thromboembolism
- PMID: 35731524
- PMCID: PMC9218925
- DOI: 10.1001/jamasurg.2022.2214
Association of Changes in Antithrombin Activity Over Time With Responsiveness to Enoxaparin Prophylaxis and Risk of Trauma-Related Venous Thromboembolism
Abstract
Importance: Venous thromboembolism (VTE) affects 2% to 20% of recovering trauma patients, despite aggressive prophylaxis with enoxaparin. Antithrombin is a primary circulating anticoagulant and crucial component of enoxaparin thromboprophylaxis. Approximately 20% of trauma patients present with antithrombin deficiency (antithrombin activity <80%).
Objective: To examine time-dependent changes in antithrombin activity, responsiveness to enoxaparin, as measured by anti-factor Xa (anti-FXa) levels, and incidence of VTE after severe trauma and to assess the association of ex vivo antithrombin supplementation with patients' sensitivity to enoxaparin prophylaxis.
Design, setting, and participants: This single-center, prospective cohort study was performed at a level 1 trauma center between January 7, 2019, and February 28, 2020. Adult trauma patients admitted to the trauma service at high risk for VTE, based on injury pattern and severity, were screened and enrolled. Patients who were older than 70 years, were pregnant, had a known immunologic or coagulation disorder, or were receiving prehospital anticoagulants were excluded.
Exposures: Blood samples were collected on emergency department arrival and daily for the first 8 days of hospitalization.
Main outcomes and measures: Patients' antithrombin activity and anti-FXa levels were measured by a coagulation analyzer, and thrombin generation was measured by calibrated automated thrombography. Responsiveness to enoxaparin was assessed by measuring anti-FXa levels 4 to 6 hours after the first daily enoxaparin dose and compared between patients who developed VTE and who did not. In addition, the associations of ex vivo supplementation of antithrombin with plasma anti-FXa levels were assessed.
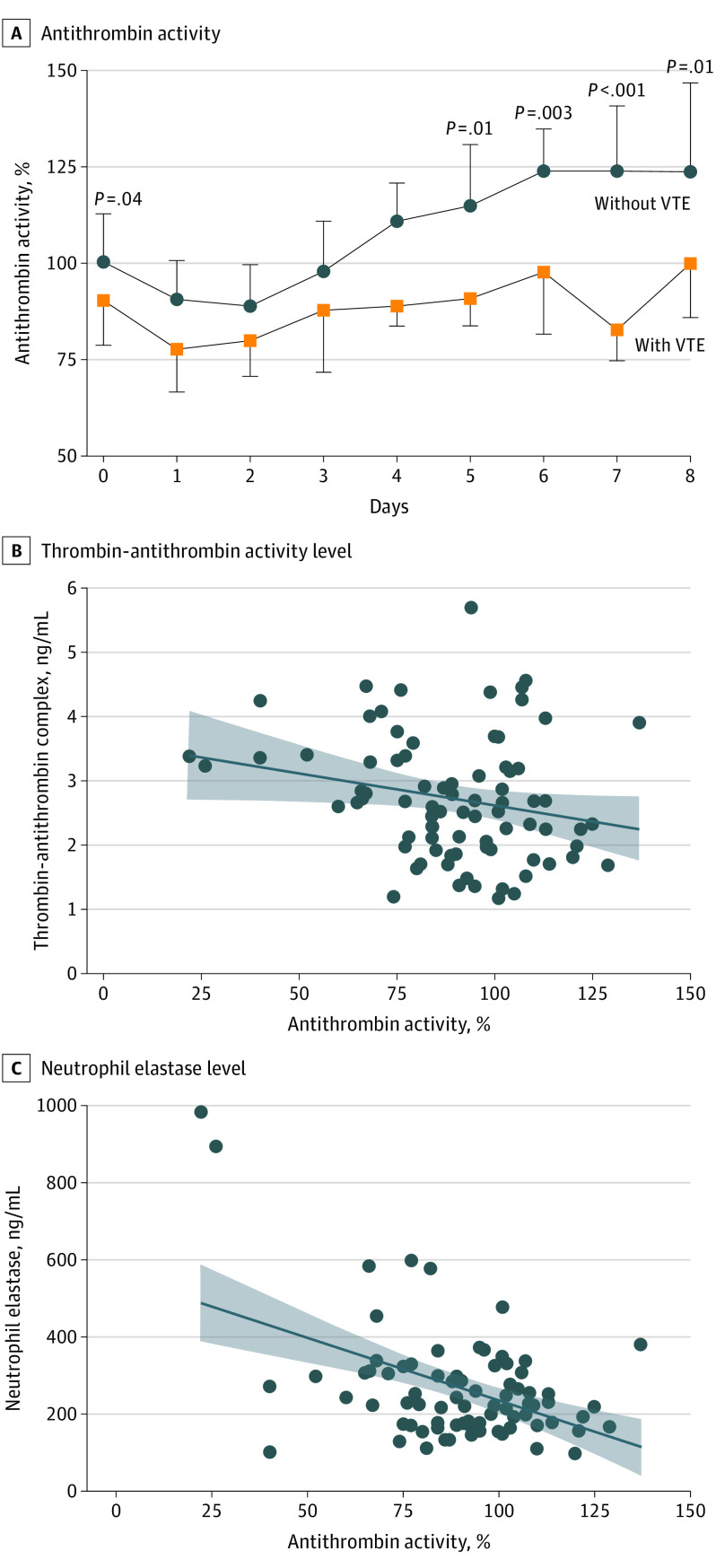
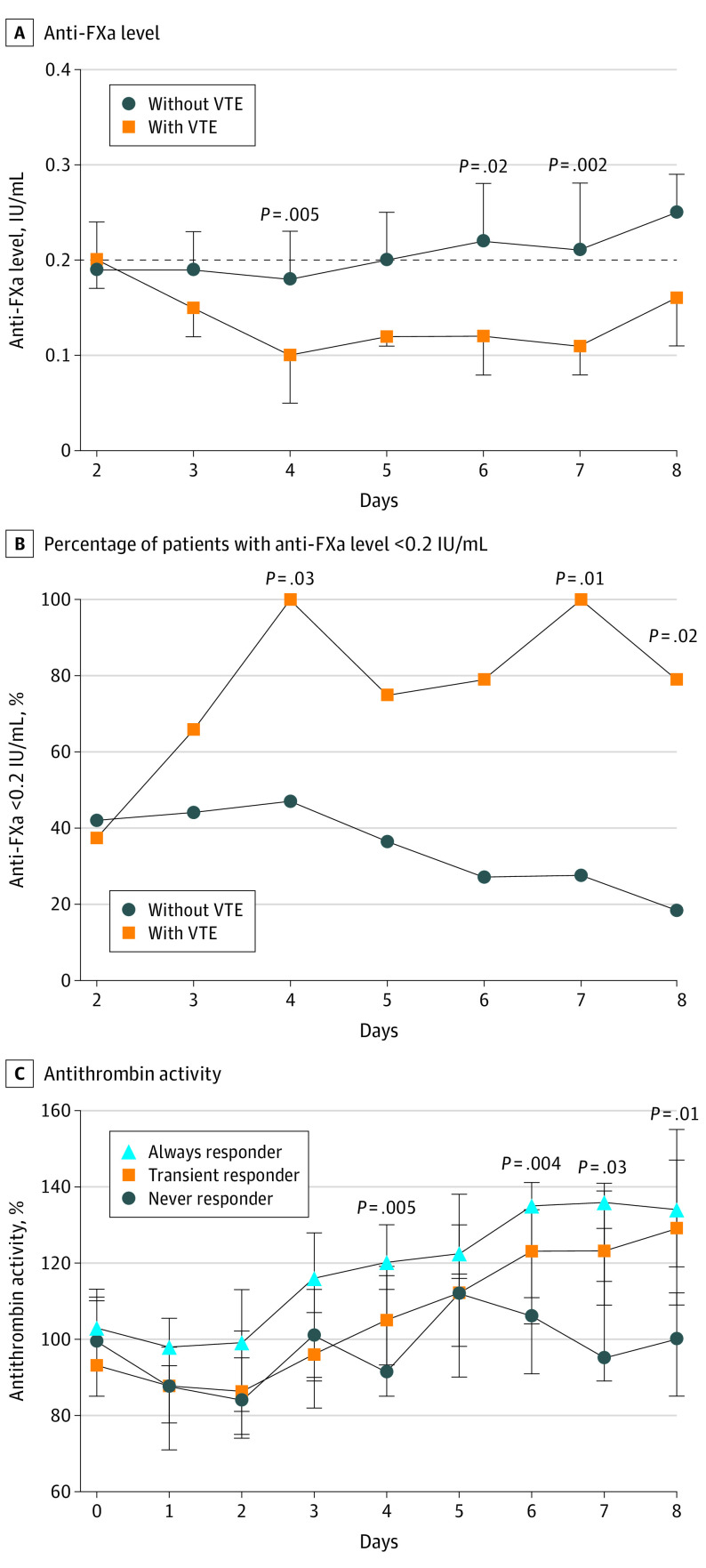
Results: Among 150 patients enrolled (median [IQR] age, 35 [27-53] years; 37 [24.7%] female and 113 [75.3%] male; 5 [3.3%] Asian, 32 [21.3%] Black, and 113 [75.3%] White; and 51 [34.0%] of Hispanic ethnicity), 28 (18.7%) developed VTE. Patients with VTE had significantly lower antithrombin activity on admission compared with patients without VTE (median [IQR], 91% [79%-104%] vs 100% [88%-112%]; P = .04), as well as lower antithrombin activity on hospital days 5 (median (IQR), 90% [83%-99%] vs 114% [99%-130%]; P = .011), 6 (median [IQR], 97% [81%-109%] vs 123% [104%-134%]; P = .003), 7 (median [IQR], 82% [74%-89%] vs 123% [110%-140%]; P < .001), and 8 (median [IQR], 99% [85%-100%] vs 123% [109%-146%]; P = .011). Anti-FXa levels were significantly lower in patients with VTE vs those without VTE at hospital day 4 (median [IQR], 0.10 [0.05-0.14] IU/mL vs 0.18 [0.13-0.23] IU/mL; P = .006), day 6 (median [IQR], 0.12 [0.08-0.14] IU/mL vs 0.22 [0.13-0.28] IU/mL; P = .02), and day 7 (median [IQR], 0.11 [0.08-0.12] IU/mL vs 0.21 [0.13, 0.28] IU/mL; P = .002). Multivariable analyses found that for every 10% decrease in antithrombin activity during the first 3 days, the risk of VTE increased 1.5-fold.
Conclusions and relevance: The results of this cohort study suggest that after severe trauma, antithrombin deficiency is common and contributes to enoxaparin resistance and VTE. Interventional studies are necessary to determine the efficacy of antithrombin supplementation in the reduction of VTE incidence.
Conflict of interest statement
Figures

Comment in
-
A Personalized Approach to Prevention of Venous Thromboembolism: One Size Does Not Fit All.JAMA Surg. 2022 Aug 1;157(8):722. doi: 10.1001/jamasurg.2022.2204. JAMA Surg. 2022. PMID: 35731539 No abstract available.
-
Targeting Chemoprophylaxis in Venous Thromboembolism Using Biomarker Guidance-Reply.JAMA Surg. 2023 Feb 1;158(2):221-222. doi: 10.1001/jamasurg.2022.5336. JAMA Surg. 2023. PMID: 36416852 No abstract available.
-
Targeting Chemoprophylaxis in Venous Thromboembolism Using Biomarker Guidance.JAMA Surg. 2023 Feb 1;158(2):220-221. doi: 10.1001/jamasurg.2022.5333. JAMA Surg. 2023. PMID: 36416853 No abstract available.
