

The Aim2Be mHealth Intervention for Children With Overweight or Obesity and Their Parents: Person-Centered Analyses to Uncover Digital Phenotypes
- PMID: 35731547
- PMCID: PMC9221987
- DOI: 10.2196/35285
The Aim2Be mHealth Intervention for Children With Overweight or Obesity and Their Parents: Person-Centered Analyses to Uncover Digital Phenotypes
Abstract
Background: Despite the growing number of mobile health (mHealth) interventions targeting childhood obesity, few studies have characterized user typologies derived from individuals' patterns of interactions with specific app features (digital phenotypes).
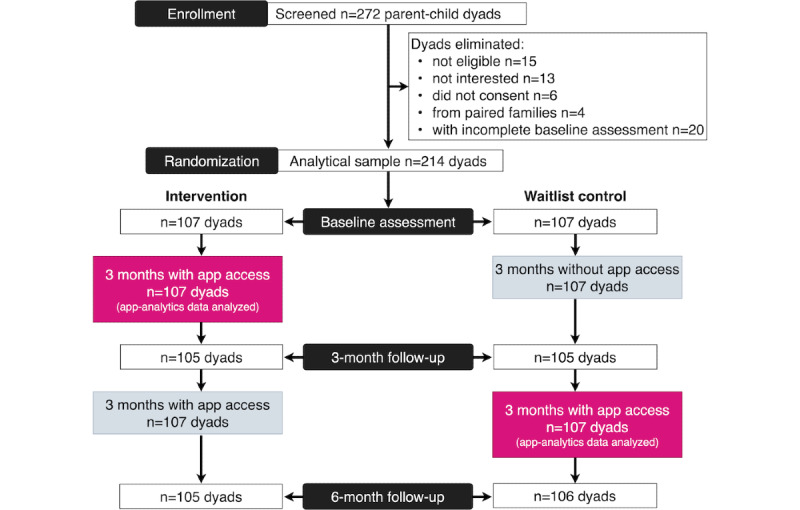
Objective: This study aims to identify digital phenotypes among 214 parent-child dyads who used the Aim2Be mHealth app as part of a randomized controlled trial conducted between 2019 and 2020, and explores whether participants' characteristics and health outcomes differed across phenotypes.
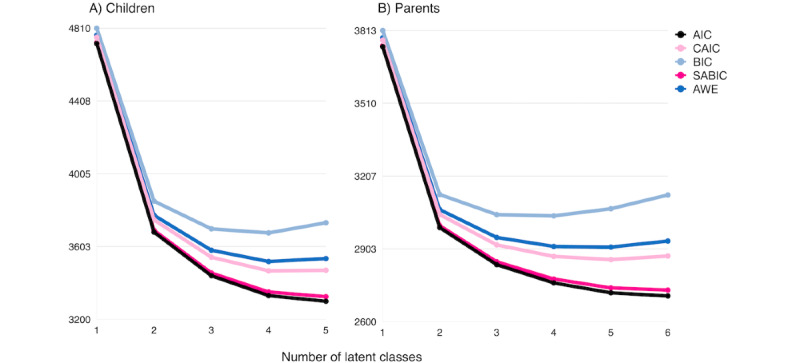
Methods: Latent class analysis was used to identify distinct parent and child phenotypes based on their use of the app's behavioral, gamified, and social features over 3 months. Multinomial logistic regression models were used to assess whether the phenotypes differed by demographic characteristics. Covariate-adjusted mixed-effect models evaluated changes in BMI z scores (zBMI), diet, physical activity, and screen time across phenotypes.
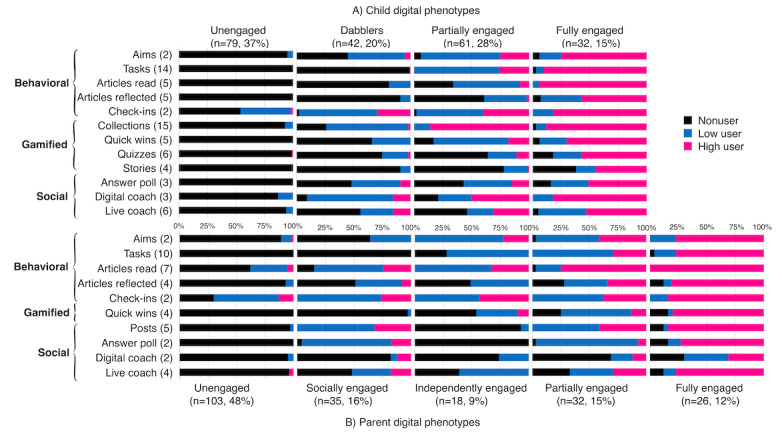
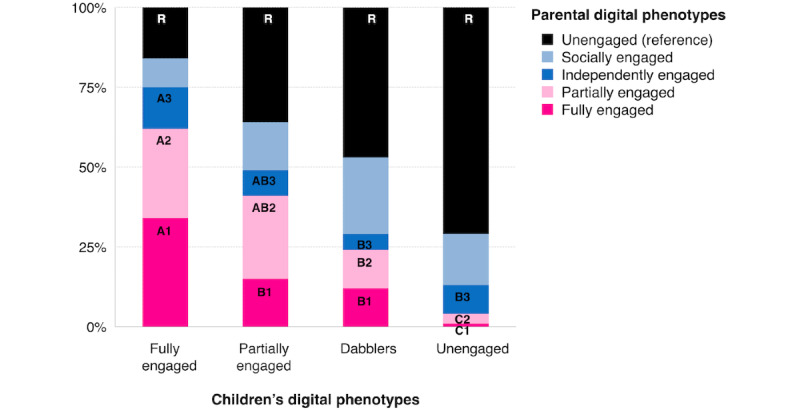
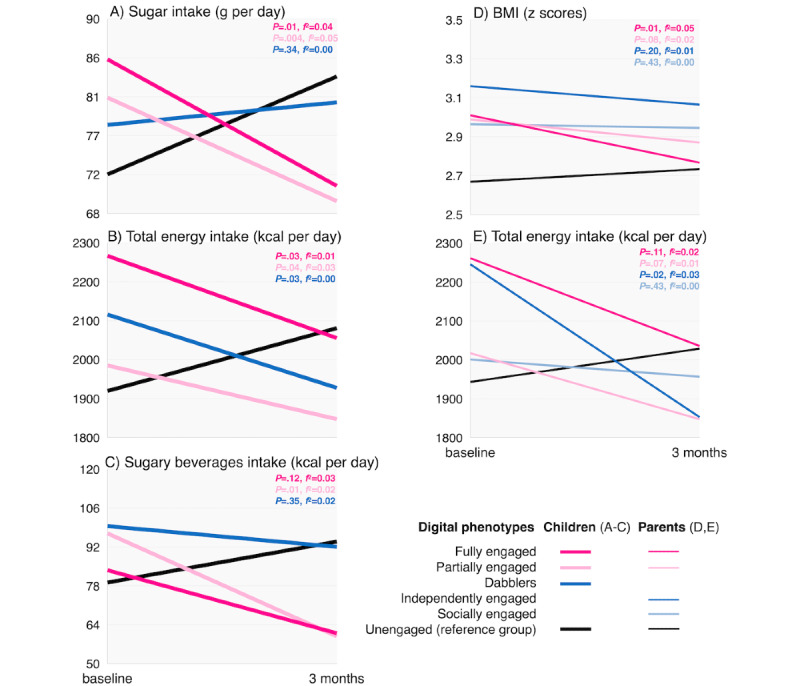
Results: Among parents, 5 digital phenotypes were identified: socially engaged (35/214, 16.3%), independently engaged (18/214, 8.4%) (socially and independently engaged parents are those who used mainly the social or the behavioral features of the app, respectively), fully engaged (26/214, 12.1%), partially engaged (32/214, 15%), and unengaged (103/214, 48.1%) users. Married parents were more likely to be fullyengaged than independently engaged (P=.02) or unengaged (P=.01) users. Socially engaged parents were older than fullyengaged (P=.02) and unengaged (P=.01) parents. The latent class analysis revealed 4 phenotypes among children: fully engaged (32/214, 15%), partially engaged (61/214, 28.5%), dabblers (42/214, 19.6%), and unengaged (79/214, 36.9%) users. Fully engaged children were younger than dabblers (P=.04) and unengaged (P=.003) children. Dabblers lived in higher-income households than fully and partiallyengaged children (P=.03 and P=.047, respectively). Fully engaged children were more likely to have fully engaged (P<.001) and partiallyengaged (P<.001) parents than unengaged children. Compared with unengaged children, fully and partiallyengaged children had decreased total sugar (P=.006 and P=.004, respectively) and energy intake (P=.03 and P=.04, respectively) after 3 months of app use. Partially engaged children also had decreased sugary beverage intake compared with unengaged children (P=.03). Similarly, children with fully engaged parents had decreased zBMI, whereas children with unengaged parents had increased zBMI over time (P=.005). Finally, children with independently engaged parents had decreased caloric intake, whereas children with unengaged parents had increased caloric intake over time (P=.02).
Conclusions: Full parent-child engagement is critical for the success of mHealth interventions. Further research is needed to understand program design elements that can affect participants' engagement in supporting behavior change.
Trial registration: ClinicalTrials.gov NCT03651284; https://clinicaltrials.gov/ct2/show/NCT03651284.
International registered report identifier (irrid): RR2-10.1186/s13063-020-4080-2.
Keywords: childhood obesity; digital phenotypes; latent class analysis; mHealth; mobile health.
©Olivia De-Jongh González, Claire N Tugault-Lafleur, E Jean Buckler, Jill Hamilton, Josephine Ho, Annick Buchholz, Katherine M Morrison, Geoff DC Ball, Louise C Mâsse. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 22.06.2022.
Conflict of interest statement
Conflicts of Interest: LCM received salary support to conduct this research, which was provided by the BC Children’s Hospital Research Institute. OD-JG received a postdoctoral salary from the University of British Columbia and received PhD scholarships from the National Council of Science and Technology (Conacyt) of Mexico and from Universidad Iberoamericana of Mexico City. CNT-L received a postdoctoral fellowship from the Canadian Institutes of Health Research. EJB received a postdoctoral fellowship from the BC Children’s Hospital Research Institute. GDCB received funding from an Alberta Health Services Chair in Obesity Research.
Figures

References
-
- Roberts KC, Shields M, de Groh M, Aziz A, Gilbert J. Overweight and obesity in children and adolescents: results from the 2009 to 2011 Canadian Health Measures Survey. Health Rep. 2012 Sep;23(3):37–41. http://www.statcan.gc.ca/pub/82-003-x/2012003/article/11706-eng.pdf - PubMed
-
- Kang NR, Kwack YS. An update on mental health problems and cognitive behavioral therapy in pediatric obesity. Pediatr Gastroenterol Hepatol Nutr. 2020 Jan;23(1):15–25. doi: 10.5223/pghn.2020.23.1.15. https://www.pghn.org/DOIx.php?id=10.5223/pghn.2020.23.1.15 - DOI - PMC - PubMed
-
- Guideline Development Panel for Treatment of Obesity‚ American Psychological Association Summary of the clinical practice guideline for multicomponent behavioral treatment of obesity and overweight in children and adolescents. Am Psychol. 2020;75(2):178–88. doi: 10.1037/amp0000530. https://www.apa.org/obesity-guideline/clinical-practice-guideline.pdf 2020-09435-005 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
