

Outcomes of incident patients treated with incremental haemodialysis as compared with standard haemodialysis and peritoneal dialysis
- PMID: 35731591
- PMCID: PMC9681916
- DOI: 10.1093/ndt/gfac205
Outcomes of incident patients treated with incremental haemodialysis as compared with standard haemodialysis and peritoneal dialysis
Abstract
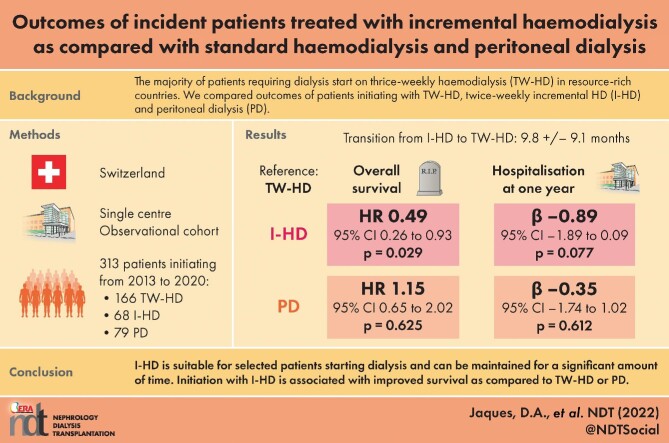
Background: Residual kidney function is considered better preserved with incremental haemodialysis (I-HD) or peritoneal dialysis (PD) as compared with conventional thrice-weekly HD (TW-HD) and is associated with improved survival. We aimed to describe outcomes of patients initiating dialysis with I-HD, TW-HD or PD.
Methods: We conducted a retrospective analysis of a prospectively assembled cohort in a single university centre including all adults initiating dialysis from January 2013 to December 2020. Primary and secondary endpoints were overall survival and hospitalization days at 1 year, respectively.
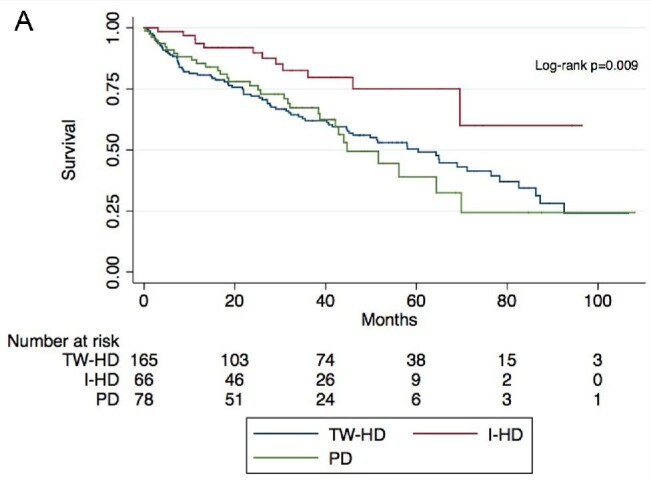
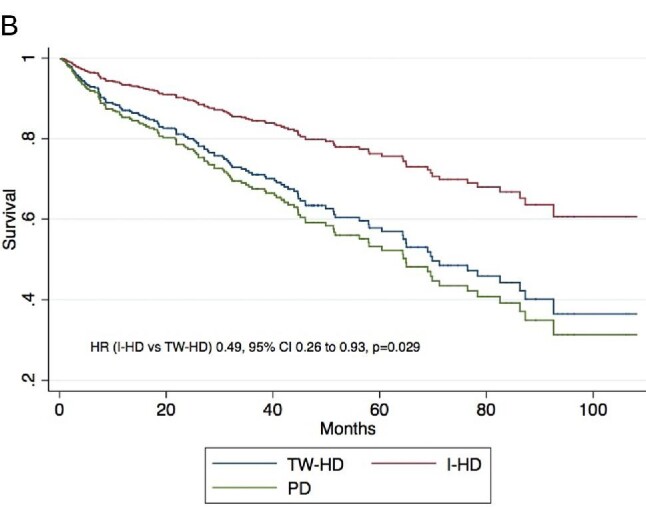
Results: We included 313 patients with 234 starting on HD (166 TW-HD and 68 I-HD) and 79 on PD. At the end of the study, 10 were still on I-HD while 45 transitioned to TW-HD after a mean duration of 9.8 ± 9.1 months. Patients who stayed on I-HD were less frequently diabetics (P = .007). Mean follow-up was 33.1 ± 30.8 months during which 124 (39.6%) patients died. Compared with patients on TW-HD, those on I-HD had improved survival (hazard ratio 0.49, 95% confidence interval 0.26-0.93, P = .029), while those on PD had similar survival. Initial kidney replacement therapy modality was not significantly associated with hospitalization days at 1 year.
Conclusions: I-HD is suitable for selected patients starting dialysis and can be maintained for a significant amount of time before transition to TW-HD, with diabetes being a risk factor. Although hospitalization days at 1 year are similar, initiation with I-HD is associated with improved survival as compared with TW-HD or PD. Results of randomized controlled trials are awaited prior to large-scale implementation of I-HD programmes.
Keywords: incremental haemodialysis; mortality; outcomes; peritoneal dialysis; survival.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures
Comment in
-
Starting chronic hemodialysis twice weekly: when less is more.Nephrol Dial Transplant. 2022 Nov 23;37(12):2297-2299. doi: 10.1093/ndt/gfac261. Nephrol Dial Transplant. 2022. PMID: 36083981 No abstract available.
References
-
- Stel VS, de Jong RW, Kramer A.et al. Supplemented ERA-EDTA Registry data evaluated the frequency of dialysis, kidney transplantation, and comprehensive conservative management for patients with kidney failure in Europe. Kidney Int 2021; 100: 182–95. Available from: https://pubmed.ncbi.nlm.nih.gov/33359055/ - PubMed
-
- Tattersall J, Dekker F, Heimbürger O.et al. When to start dialysis: updated guidance following publication of the Initiating Dialysis Early and Late (IDEAL) Study. Nephrol Dial Transplant 2011; 26: 2082–6. Available from: https://pubmed.ncbi.nlm.nih.gov/21551086/ - PubMed
-
- Shafi T, Jaar BG, Plantinga LC.et al. Association of residual urine output with mortality, quality of life, and inflammation in incident hemodialysis patients: the Choices for Healthy Outcomes in Caring for End-Stage Renal Disease (CHOICE) Study. Am J Kidney Dis 2010; 56: 348–58. Available from: https://pubmed.ncbi.nlm.nih.gov/20605303/ - PMC - PubMed
-
- Eknoyan G, Beck GJ, Cheung AK.et al. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med 2002; 347: 2010–19. Available from: https://pubmed.ncbi.nlm.nih.gov/12490682/ - PubMed
-
- Gotch FA, Sargent JA.. A mechanistic analysis of the National Cooperative Dialysis Study (NCDS). Kidney Int 1985; 28: 526–34. Available from: https://pubmed.ncbi.nlm.nih.gov/3934452/ - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
