

Beta-Lactam Antibiotic Therapeutic Drug Monitoring in Critically Ill Patients: A Systematic Review and Meta-Analysis
- PMID: 35731853
- PMCID: PMC9662173
- DOI: 10.1093/cid/ciac506
Beta-Lactam Antibiotic Therapeutic Drug Monitoring in Critically Ill Patients: A Systematic Review and Meta-Analysis
Abstract
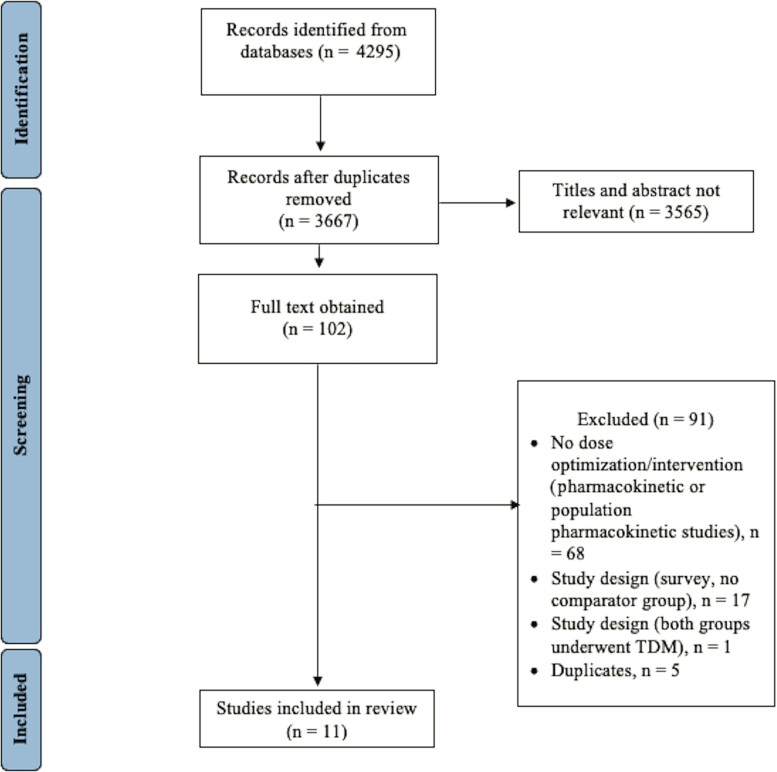
Therapeutic drug monitoring (TDM) of beta-lactam antibiotics is recommended to address the variability in exposure observed in critical illness. However, the impact of TDM-guided dosing on clinical outcomes remains unknown. We conducted a systematic review and meta-analysis on TDM-guided dosing and clinical outcomes (all-cause mortality, clinical cure, microbiological cure, treatment failure, hospital and intensive care unit length of stay, target attainment, antibiotic-related adverse events, and emergence of resistance) in critically ill patients with suspected or proven sepsis. Eleven studies (n = 1463 participants) were included. TDM-guided dosing was associated with improved clinical cure (relative risk, 1.17; 95% confidence interval [CI], 1.04 to 1.31), microbiological cure (RR, 1.14; 95% CI, 1.03 to 1.27), treatment failure (RR, 0.79; 95% CI, .66 to .94), and target attainment (RR, 1.85; 95% CI, 1.08 to 3.16). No associations with mortality and length of stay were found. TDM-guided dosing improved clinical and microbiological cure and treatment response. Larger, prospective, randomized trials are required to better assess the utility of beta-lactam TDM in critically ill patients.
Keywords: antibacterial agents; critical illness; drug concentration; pharmacodynamics; pharmacokinetics.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. R. P. M. reports a doctorate support scholarship from the National Health and Medical Research Council of Australia (NHMRC) unrelated to this work. A. A. U. reports grant funding from the NHMRC (paid to Monash University), the Medical Research Future Fund (MRFF) Australia (paid to Monash University), and the Department of Health, Commonwealth of Australia (paid to Monash University) for research projects outside the current work and in-kind support (trial consumables) from Integra Lifesciences for a project outside the current work. A. Y. P. reports grant funding from the NHMRC (Practitioner Fellowship; paid to Monash University) for research projects outside the current work and an investigator-initiated research grant from Merck Sharp & Dohme Corp. T. N. P. reports an NHMRC Career Development Fellowship; funds for advisory board consultancy for Merck Sharp & Dohme Corp outside the scope the submitted work and paid to author’s institution; and fees from Australian Health Unity as a consultant advising on coronavirus disease 2019 preparedness in residential aged care facilities. All authors declare that they have no known conflicts of interest, financial or otherwise that could have influenced the research reported in this paper. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures


Comment in
-
β-Lactam Therapeutic Drug Monitoring in Critically Ill Patients.Clin Infect Dis. 2023 Jun 16;76(12):2212-2213. doi: 10.1093/cid/ciad150. Clin Infect Dis. 2023. PMID: 36932040 No abstract available.
