Evaluation of Recombinant Live-Attenuated Respiratory Syncytial Virus (RSV) Vaccines RSV/ΔNS2/Δ1313/I1314L and RSV/276 in RSV-Seronegative Children
- PMID: 35732186
- PMCID: PMC10205613
- DOI: 10.1093/infdis/jiac253
Evaluation of Recombinant Live-Attenuated Respiratory Syncytial Virus (RSV) Vaccines RSV/ΔNS2/Δ1313/I1314L and RSV/276 in RSV-Seronegative Children
Abstract
Background: This United States-based study compared 2 candidate vaccines: RSV/ΔNS2/Δ1313/I1314L, attenuated by NS2 gene-deletion and temperature-sensitivity mutation in the polymerase gene; and RSV/276, attenuated by M2-2 deletion.
Methods: RSV-seronegative children aged 6-24 months received RSV/ΔNS2/Δ1313/I1314L (106 plaque-forming units [PFU]), RSV/276 (105 PFU), or placebo intranasally. Participants were monitored for vaccine shedding, reactogenicity, and RSV serum antibodies, and followed over the subsequent RSV season.
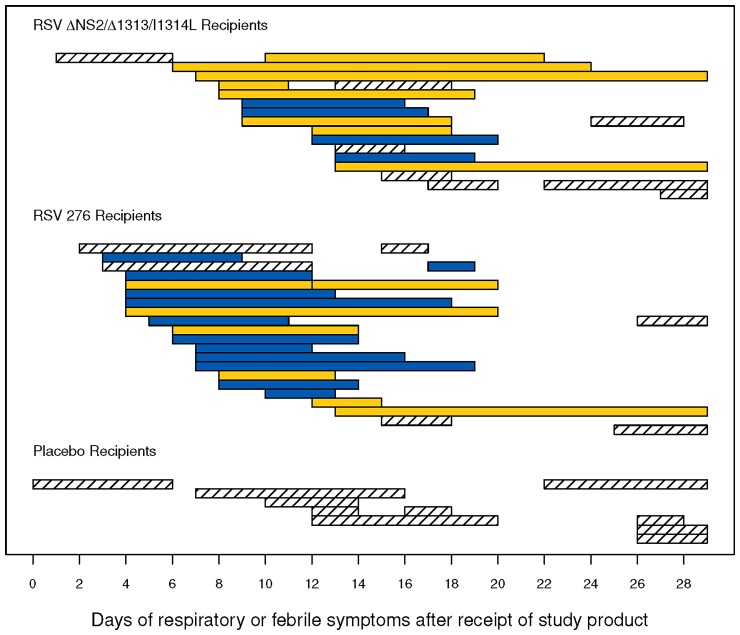
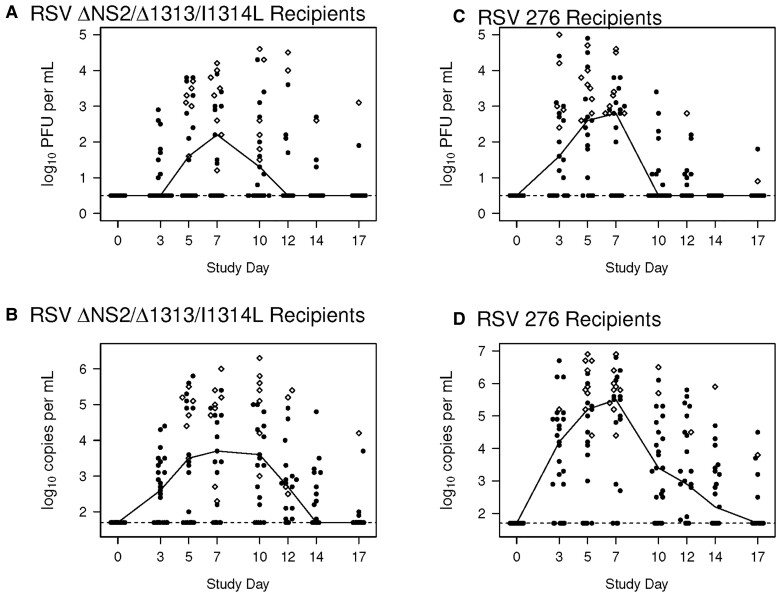
Results: Enrollment occurred September 2017 to October 2019. During 28 days postinoculation, upper respiratory illness and/or fever occurred in 64% of RSV/ΔNS2/Δ1313/I1314L, 84% of RSV/276, and 58% of placebo recipients. Symptoms were generally mild. Cough was more common in RSV/276 recipients than RSV/ΔNS2/Δ1313/I1314L (48% vs 12%; P = .012) or placebo recipients (17%; P = .084). There were no lower respiratory illness or serious adverse events. Eighty-eight and 96% of RSV/ΔNS2/Δ1313/I1314L and RSV/276 recipients were infected with vaccine (shed vaccine and/or had ≥4-fold rises in RSV antibodies). Serum RSV-neutralizing titers and anti-RSV F IgG titers increased ≥4-fold in 60% and 92% of RSV/ΔNS2/Δ1313/I1314L and RSV/276 vaccinees, respectively. Exposure to community RSV during the subsequent winter was associated with strong anamnestic RSV-antibody responses.
Conclusions: Both vaccines had excellent infectivity and were well tolerated. RSV/276 induced an excess of mild cough. Both vaccines were immunogenic and primed for strong anamnestic responses.
Clinical trials registration: NCT03227029 and NCT03422237.
Keywords: RNA regulatory protein M2-2; RSV; immunogenicity; live-attenuated viral vaccine; neutralizing antibodies; respiratory syncytial virus.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. U. J. B., C. L., and P. L. C. are listed as inventors on patents related to live-attenuated RSV vaccines, including vaccines containing genetically stabilized attenuating mutations and received research support and royalties paid by Sanofi. C. K. C. and R. A. K. have served as paid consultants to Sanofi. E. J. M. participated in an advisory board meeting for Sanofi. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures