

Integrated multi-omic characterization of congenital heart disease
- PMID: 35732239
- PMCID: PMC10405779
- DOI: 10.1038/s41586-022-04989-3
Integrated multi-omic characterization of congenital heart disease
Abstract
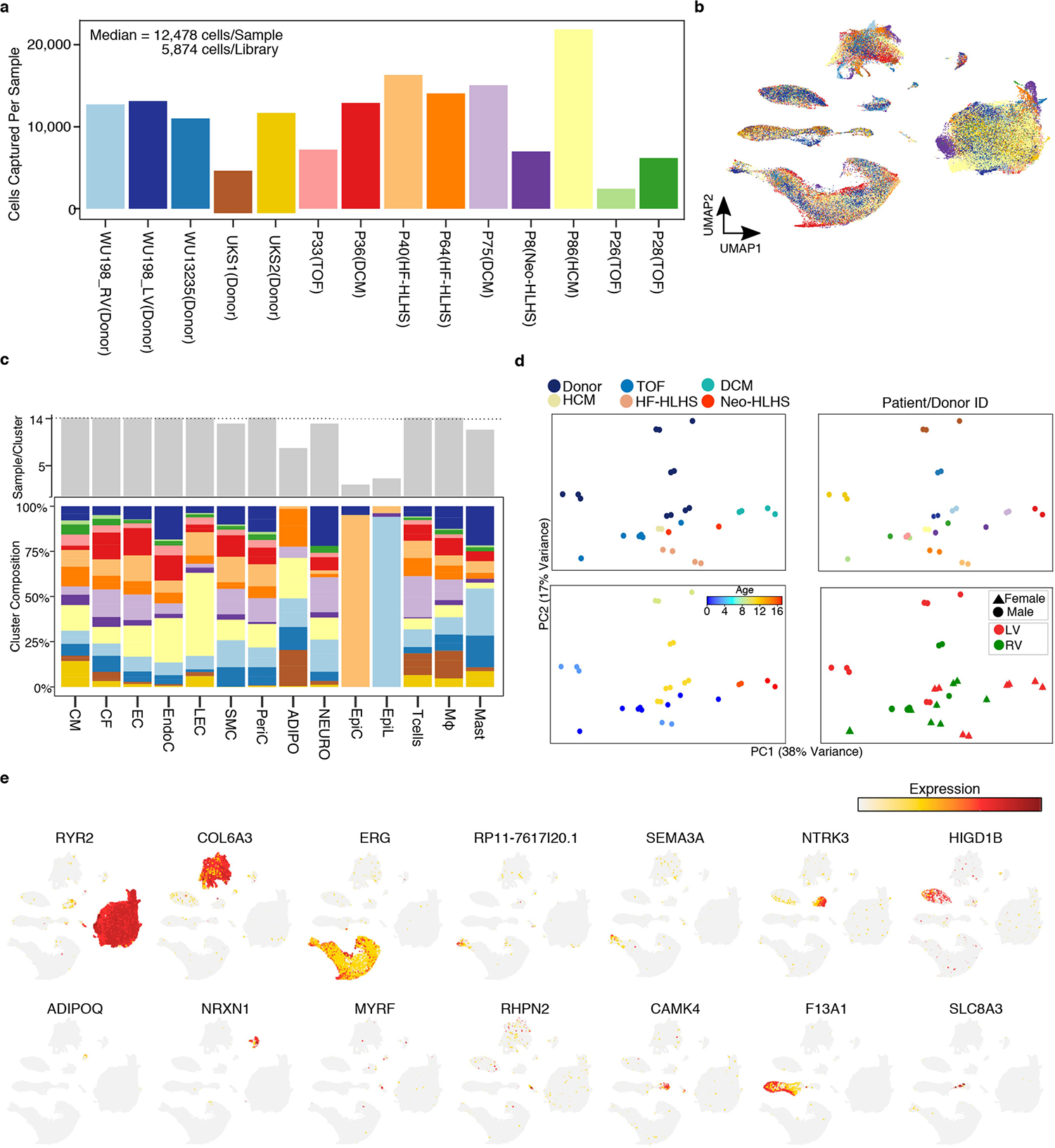
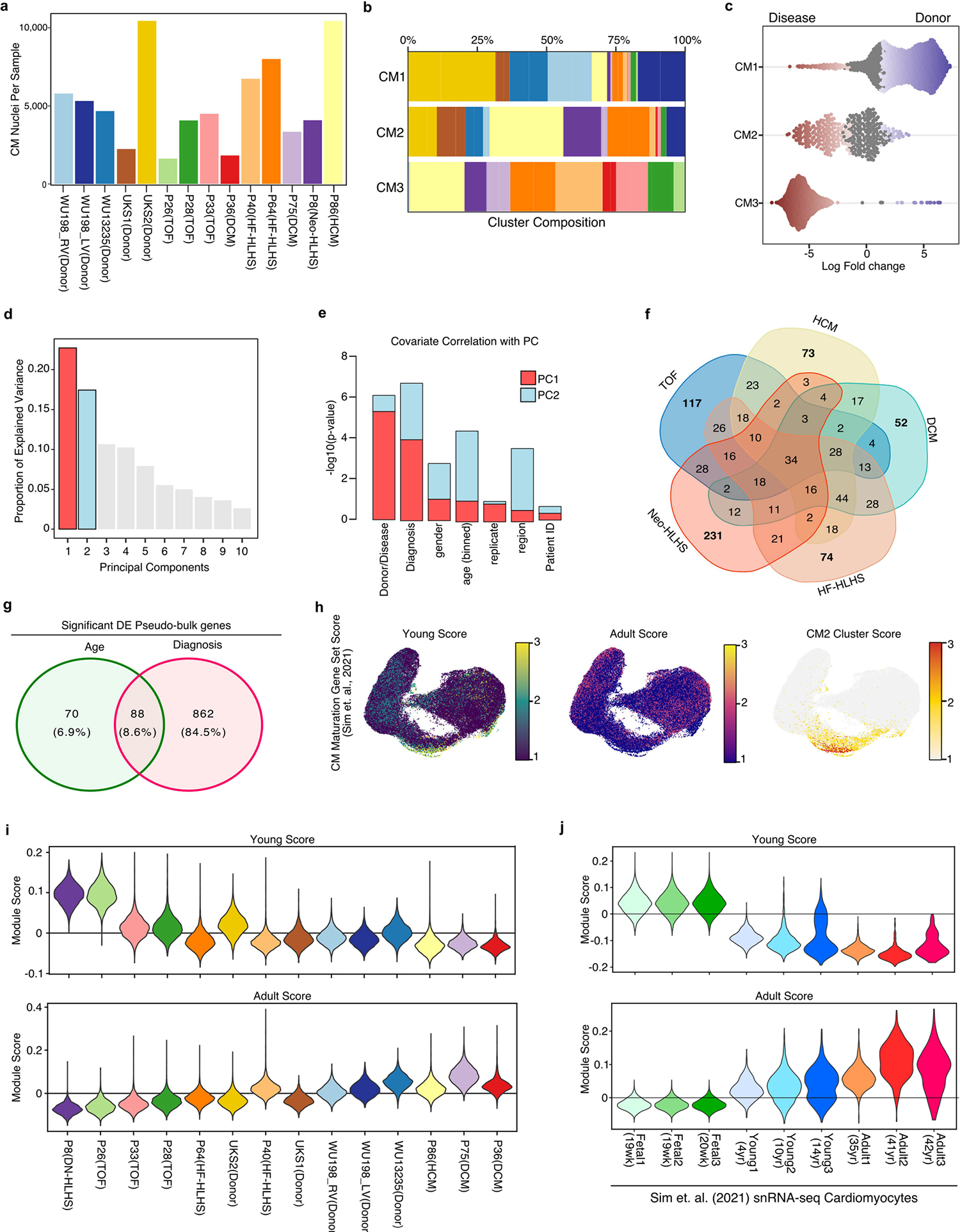
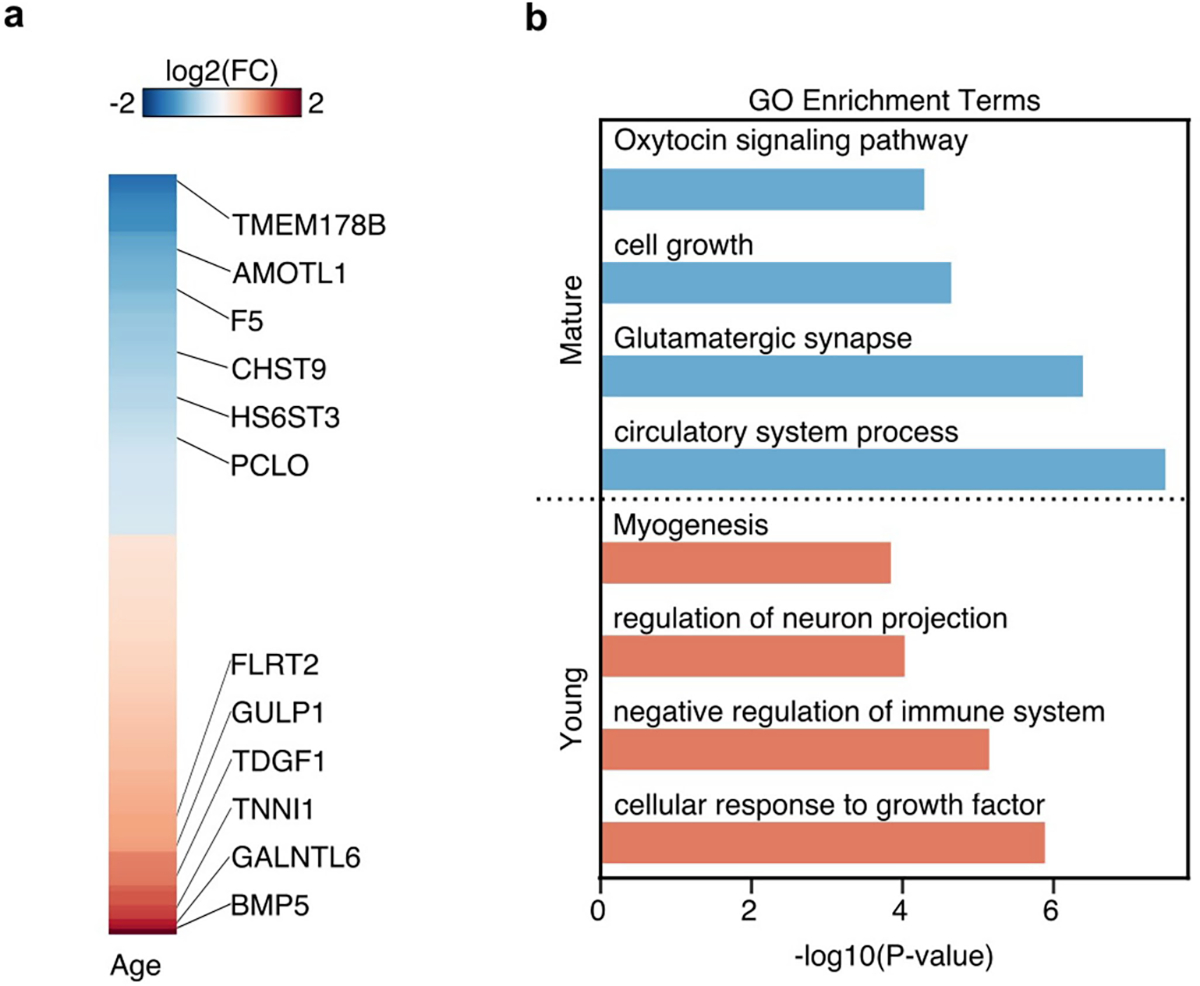
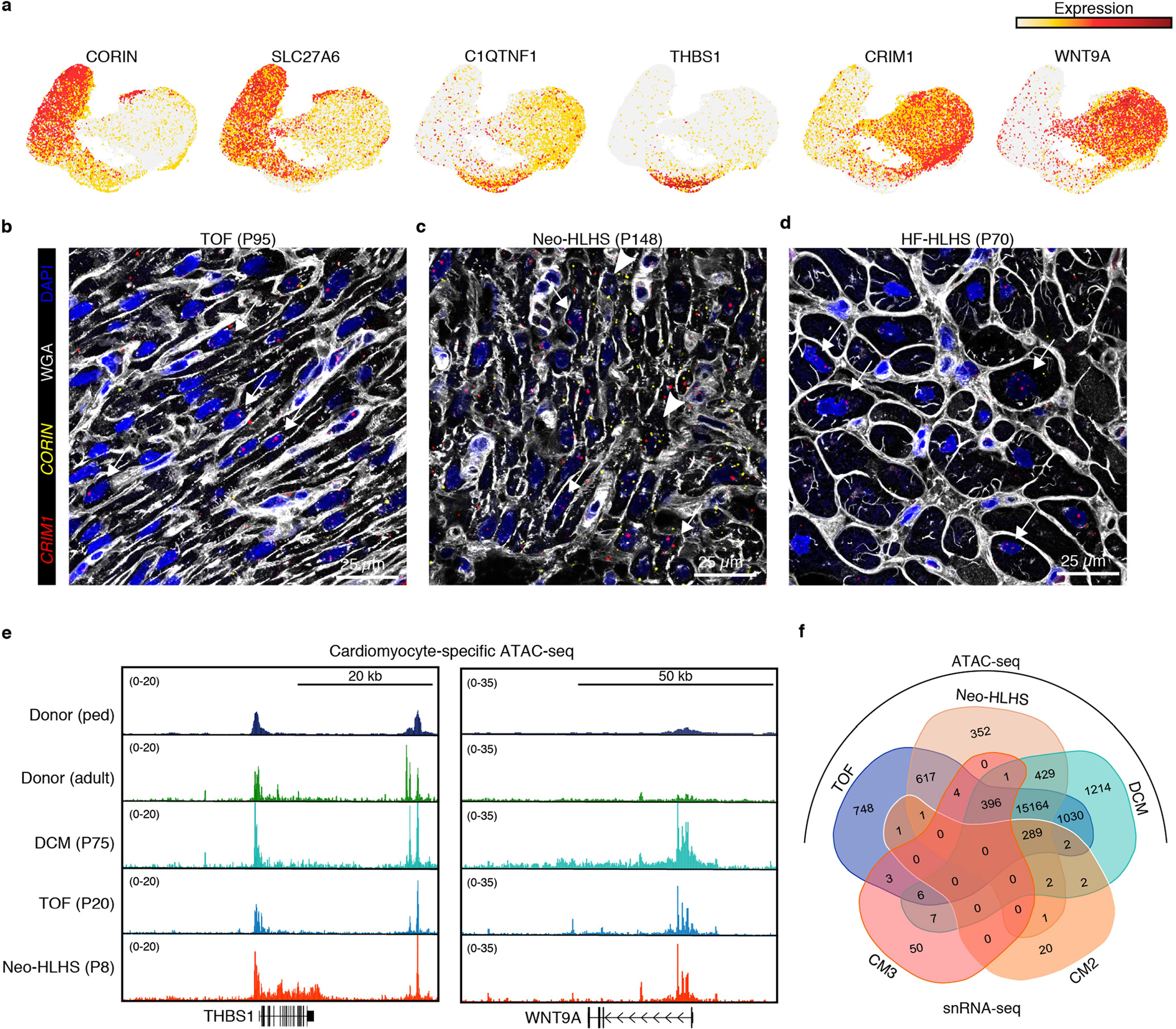
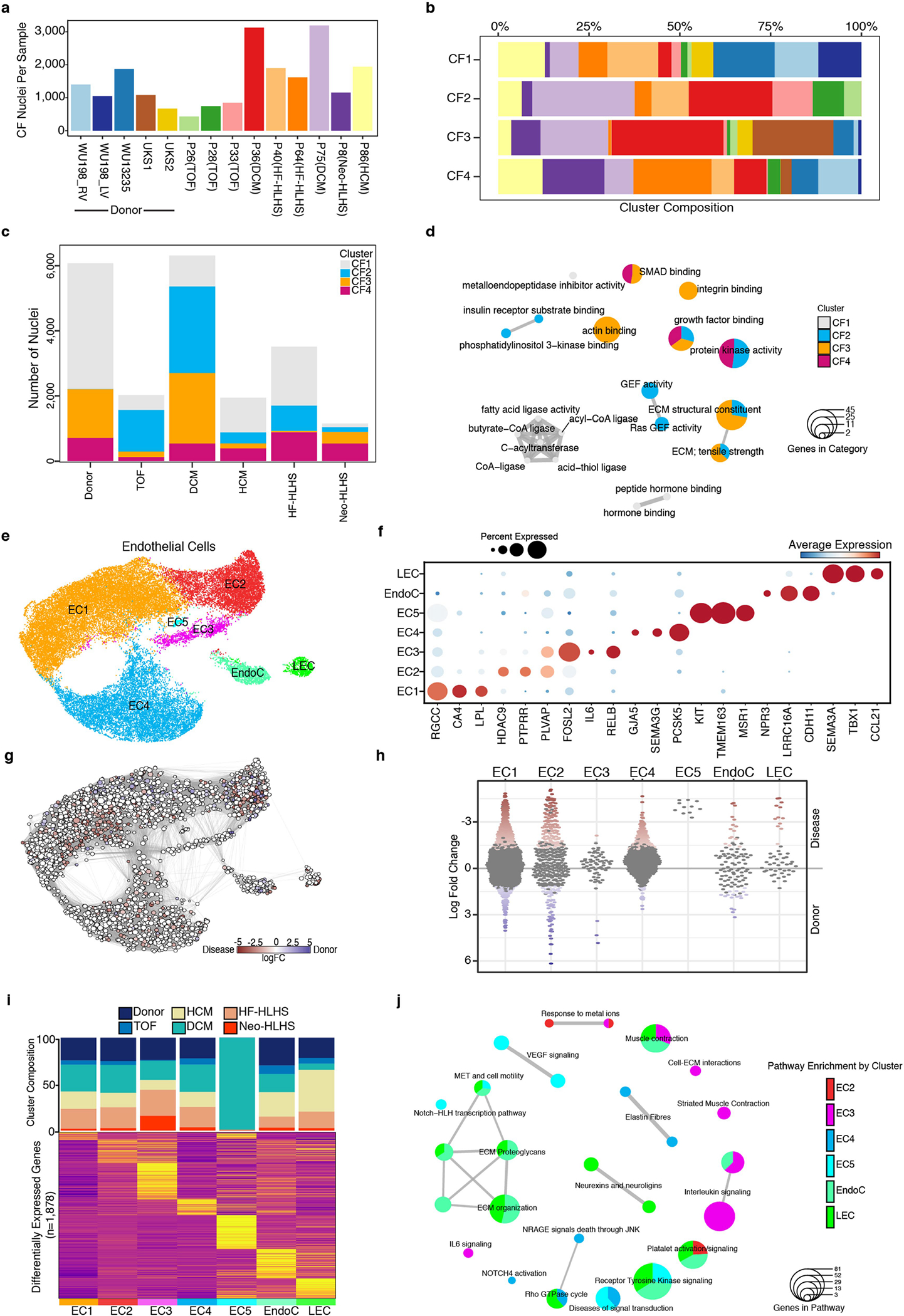
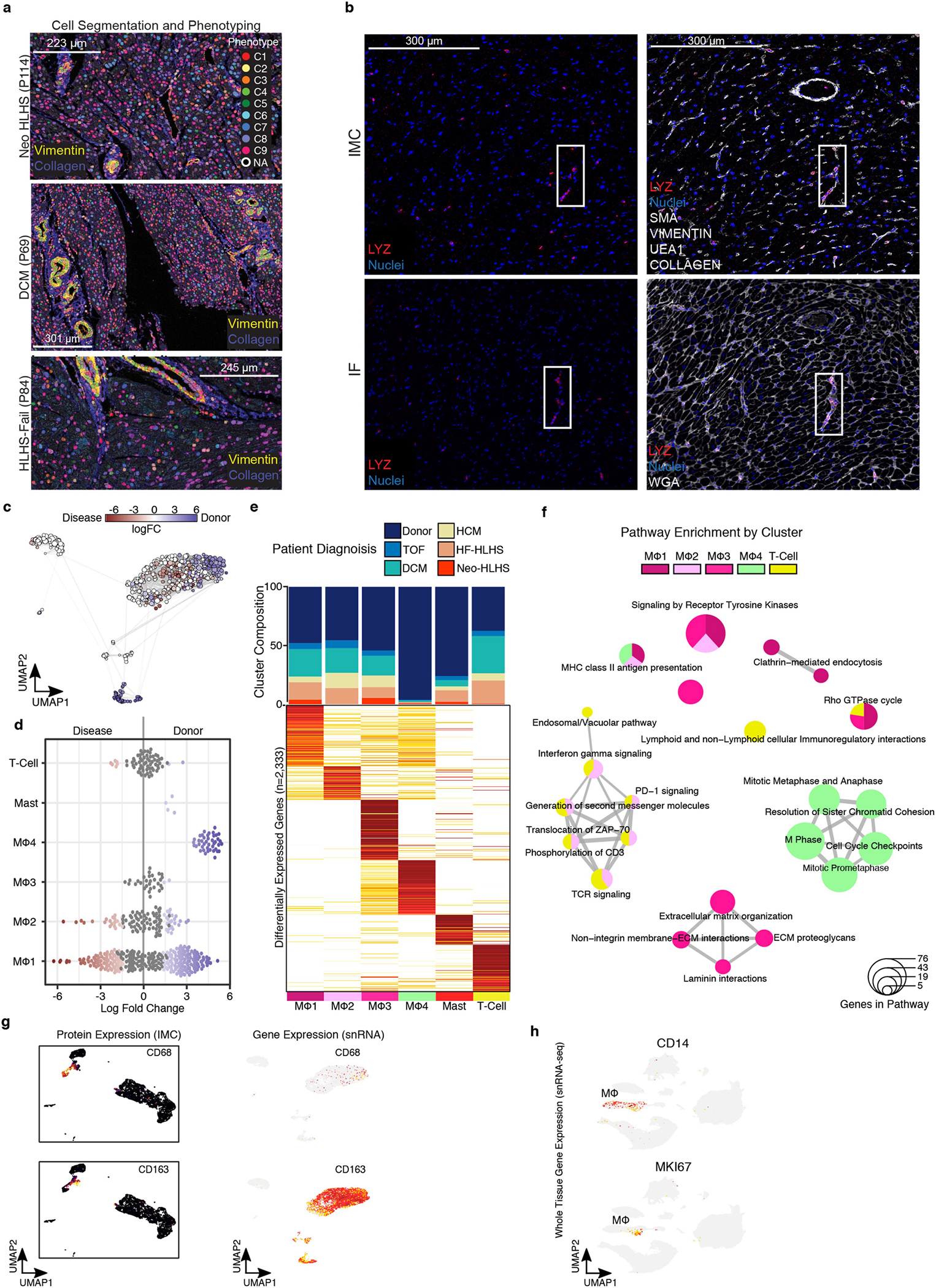
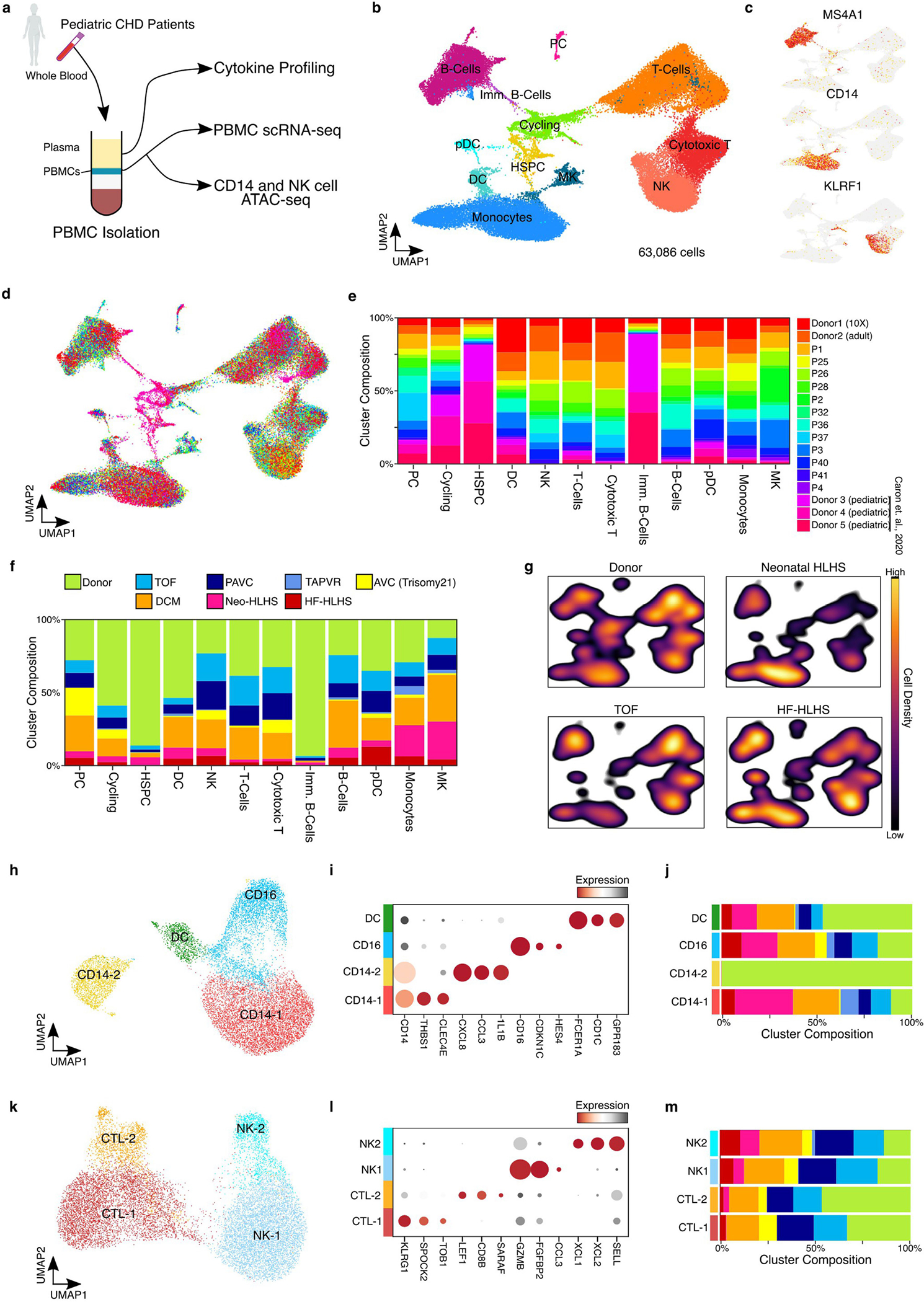
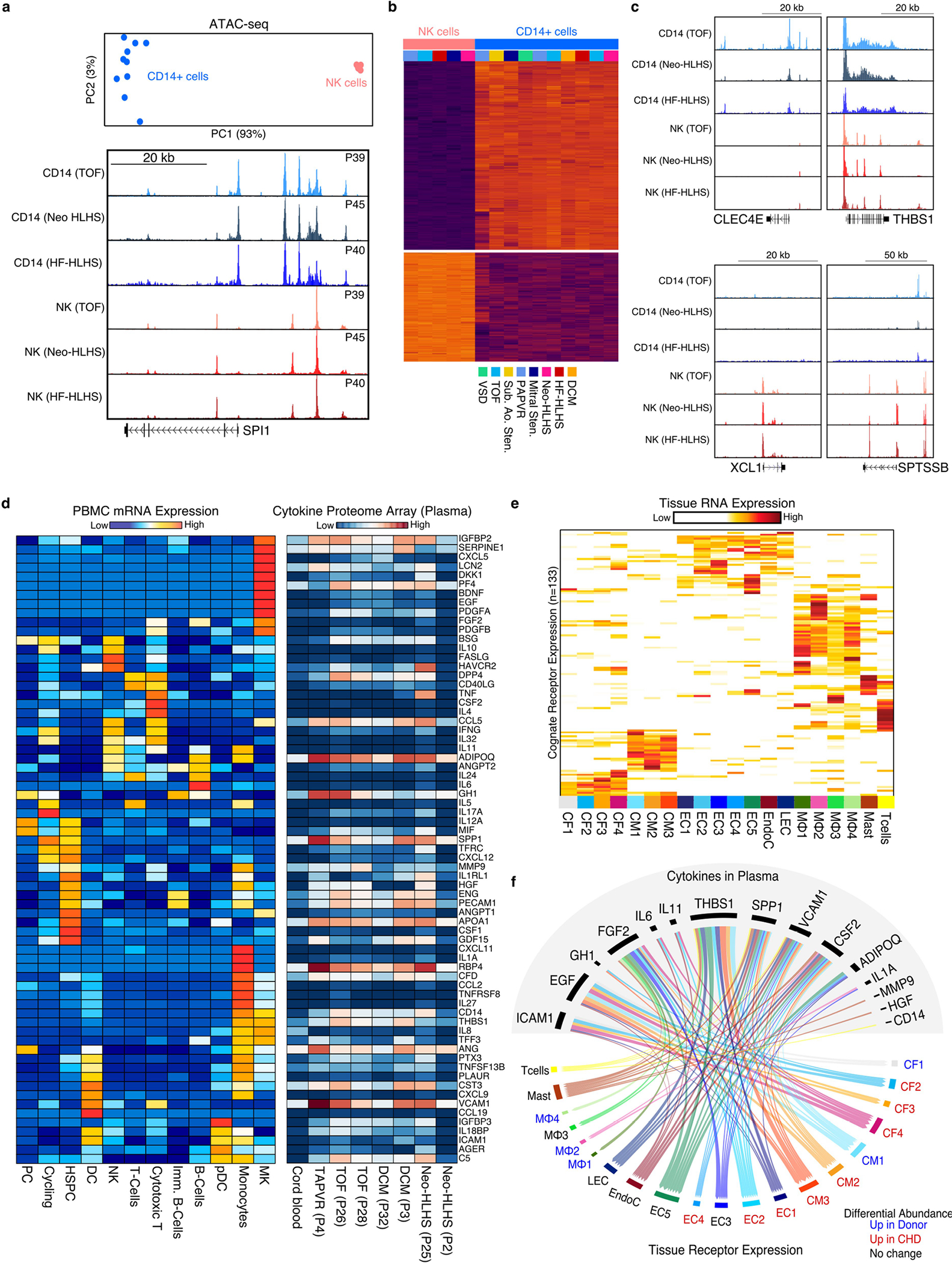
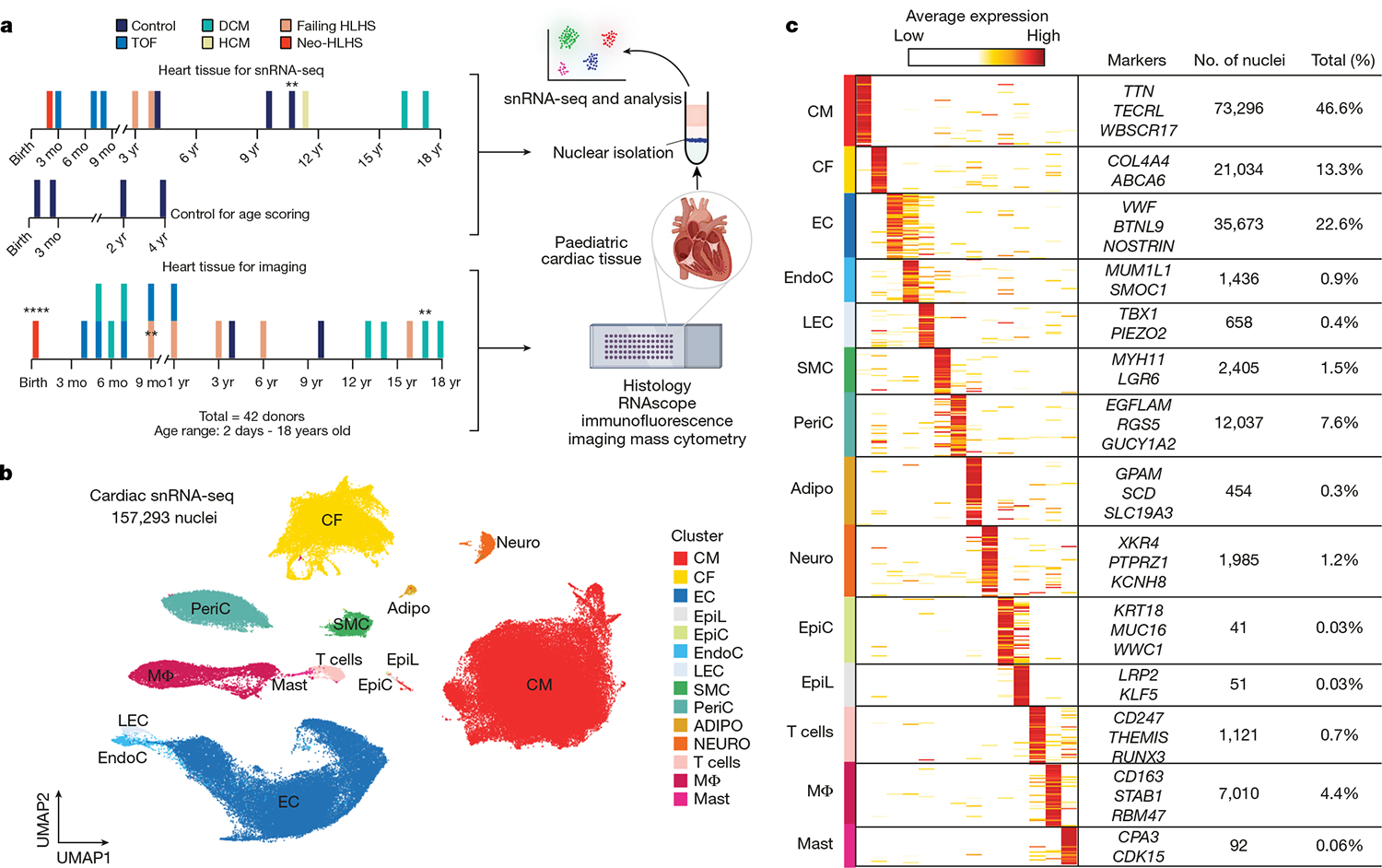
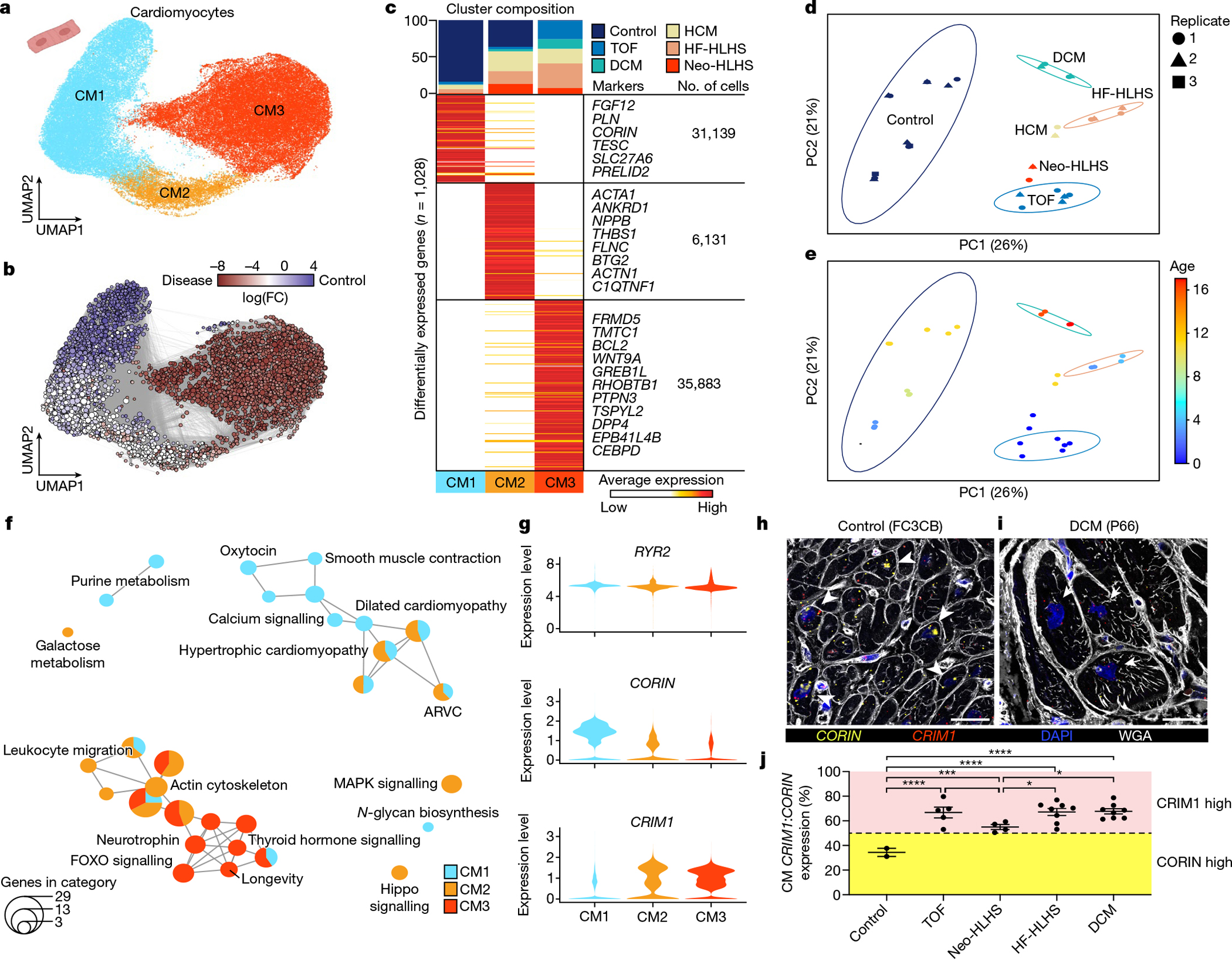
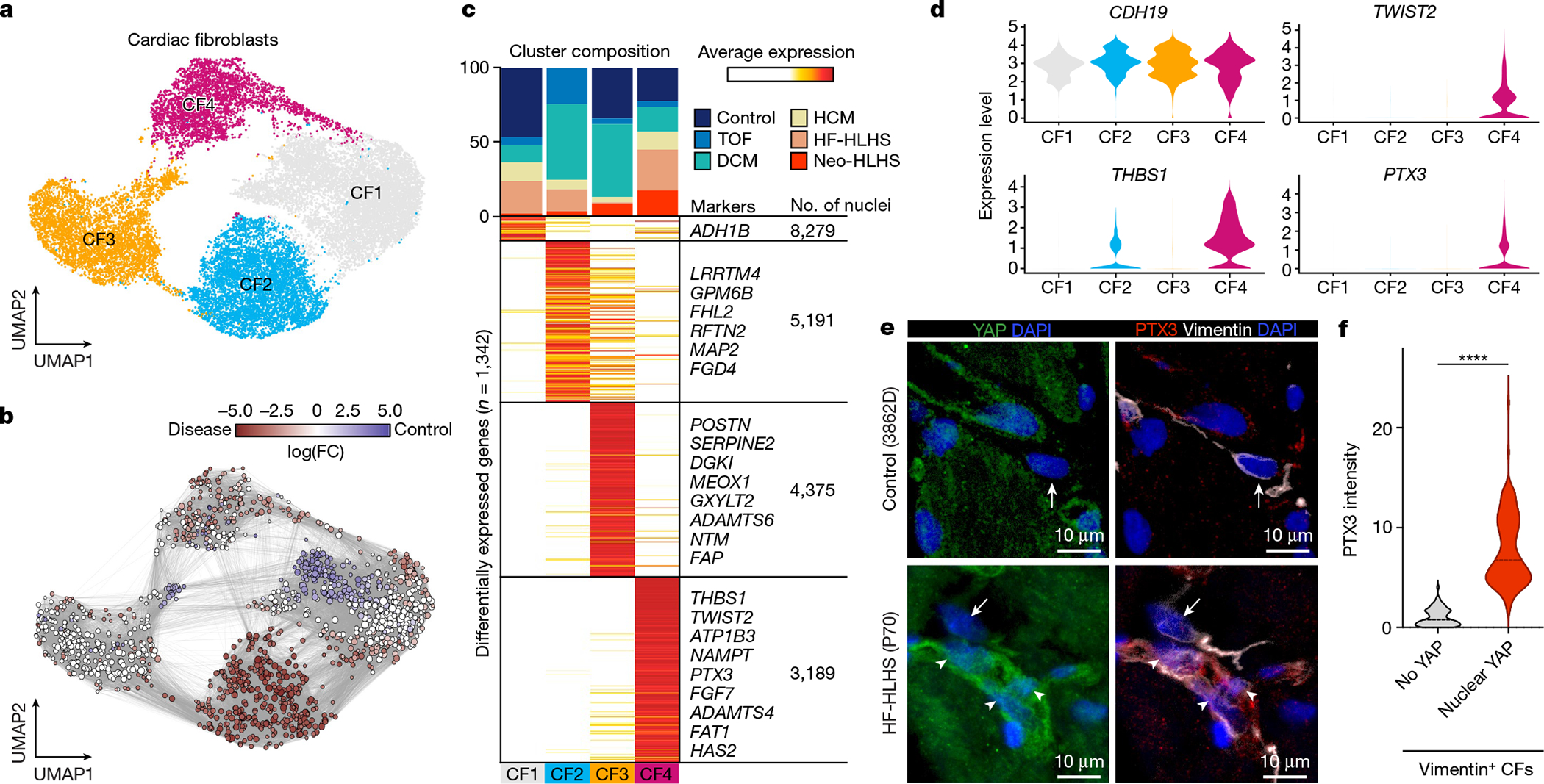
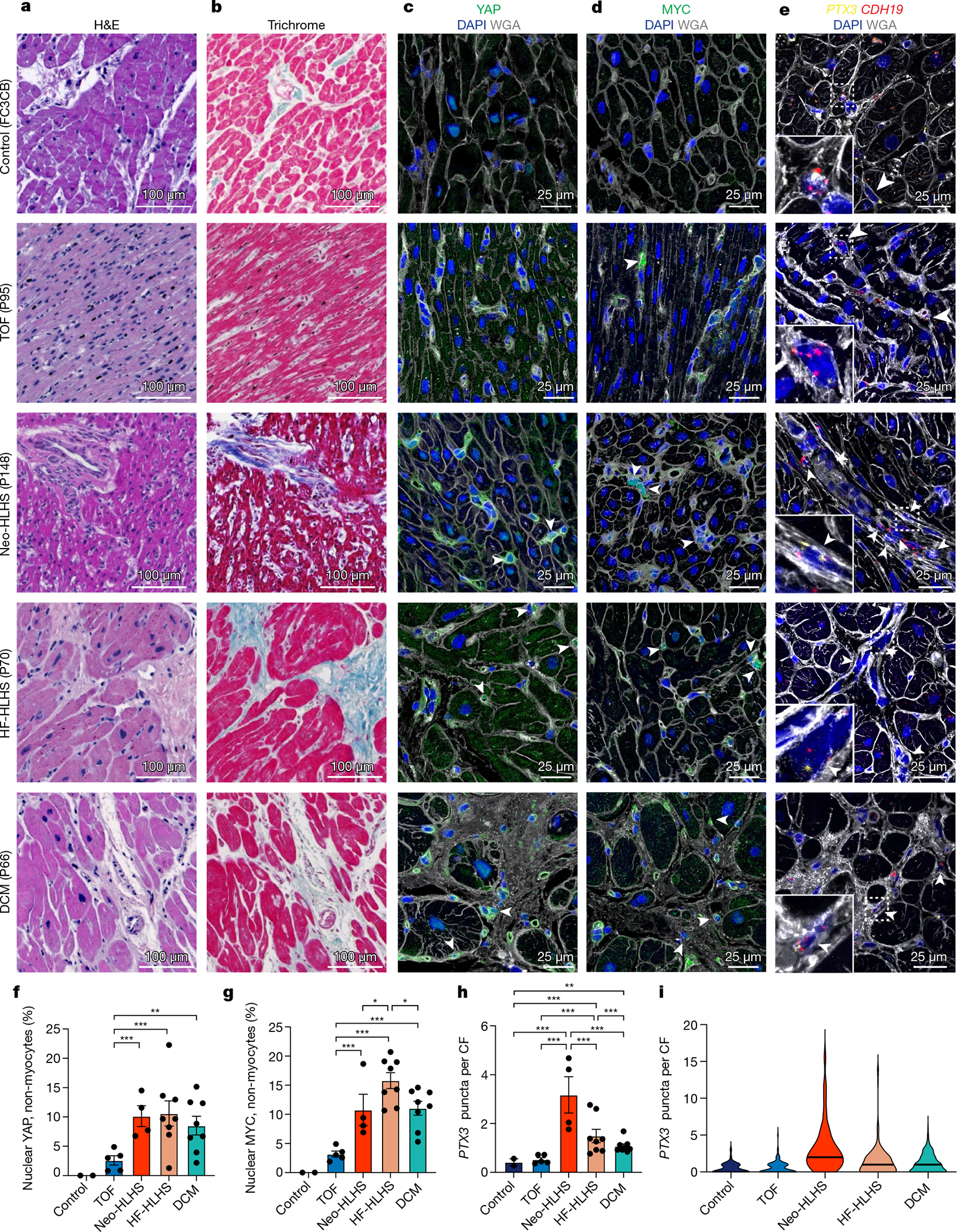
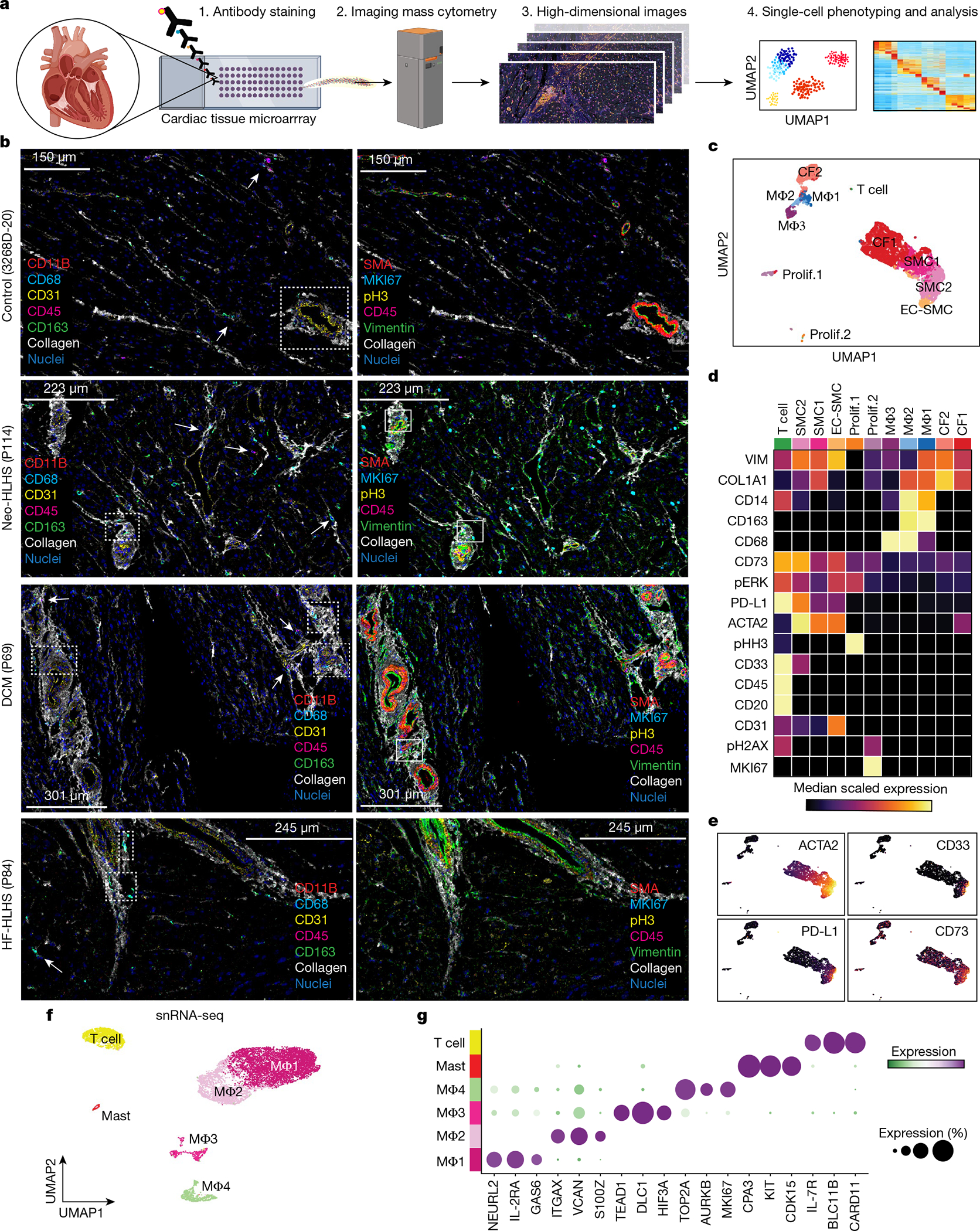
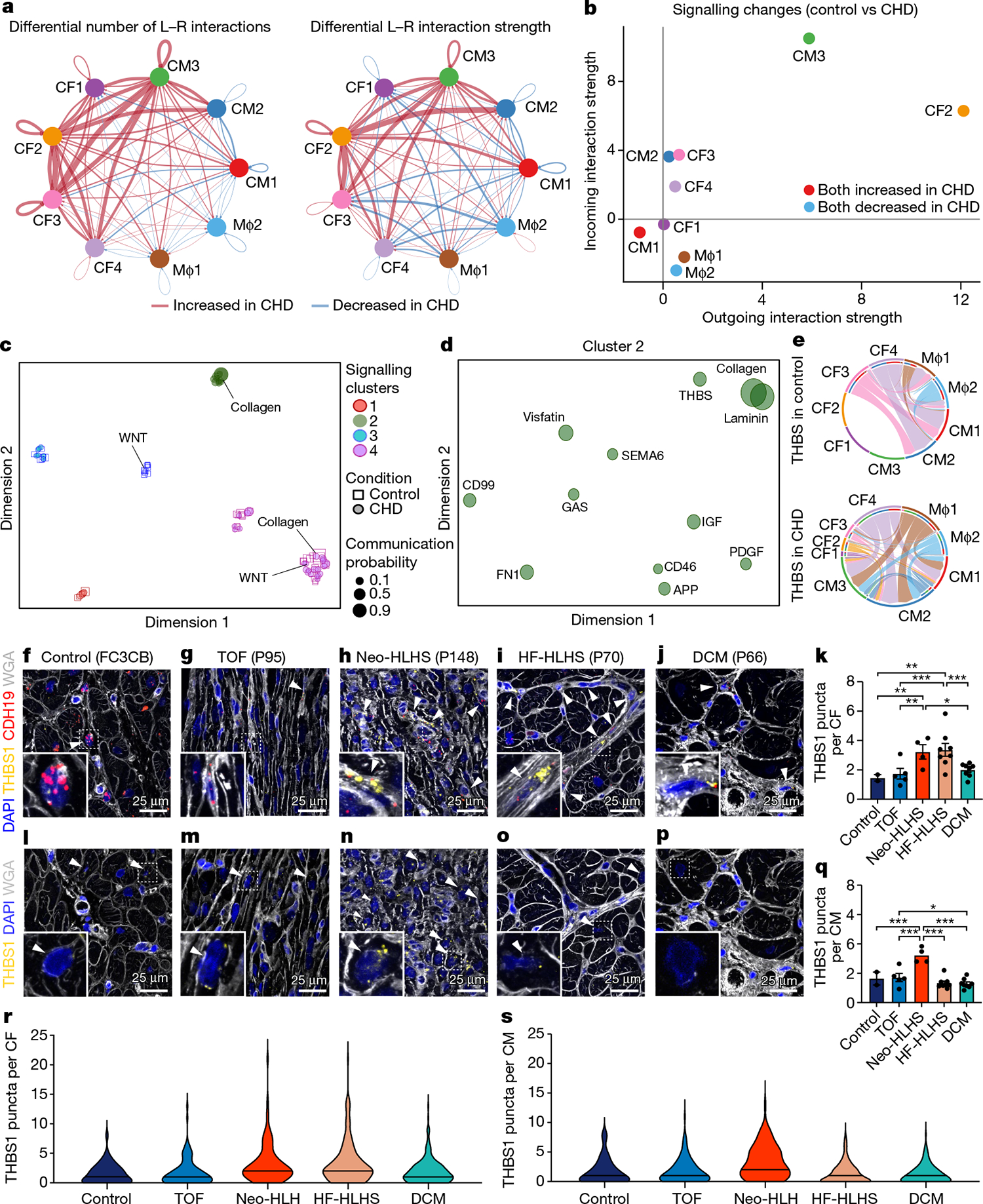
The heart, the first organ to develop in the embryo, undergoes complex morphogenesis that when defective results in congenital heart disease (CHD). With current therapies, more than 90% of patients with CHD survive into adulthood, but many suffer premature death from heart failure and non-cardiac causes1. Here, to gain insight into this disease progression, we performed single-nucleus RNA sequencing on 157,273 nuclei from control hearts and hearts from patients with CHD, including those with hypoplastic left heart syndrome (HLHS) and tetralogy of Fallot, two common forms of cyanotic CHD lesions, as well as dilated and hypertrophic cardiomyopathies. We observed CHD-specific cell states in cardiomyocytes, which showed evidence of insulin resistance and increased expression of genes associated with FOXO signalling and CRIM1. Cardiac fibroblasts in HLHS were enriched in a low-Hippo and high-YAP cell state characteristic of activated cardiac fibroblasts. Imaging mass cytometry uncovered a spatially resolved perivascular microenvironment consistent with an immunodeficient state in CHD. Peripheral immune cell profiling suggested deficient monocytic immunity in CHD, in agreement with the predilection in CHD to infection and cancer2. Our comprehensive phenotyping of CHD provides a roadmap towards future personalized treatments for CHD.
© 2022. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
Figures
Comment in
-
Single-cell profiles of CHD and CM.Nat Rev Cardiol. 2022 Sep;19(9):575. doi: 10.1038/s41569-022-00753-2. Nat Rev Cardiol. 2022. PMID: 35817872 No abstract available.
References
-
- Raissadati A, Nieminen H, Jokinen E & Sairanen H Progress in late results among pediatric cardiac surgery patients: a population-based 6-decade study with 98% follow-up. Circulation 131, 347–353 (2015). - PubMed
-
- Diller GP et al. Survival prospects and circumstances of death in contemporary adult congenital heart disease patients under follow-up at a large tertiary centre. Circulation 132, 2118–2125 (2015). - PubMed
-
- Hsu DT & Pearson GD Heart failure in children: part II: diagnosis, treatment, and future directions. Circ. Heart. Fail. 2, 490–498 (2009). - PubMed
MeSH terms
Substances
Grants and funding
- R01 HL142704/HL/NHLBI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- R01 HL118761/HL/NHLBI NIH HHS/United States
- R56 HL142704/HL/NHLBI NIH HHS/United States
- R01 HL149164/HL/NHLBI NIH HHS/United States
- R01 HL127717/HL/NHLBI NIH HHS/United States
- T32 HL007208/HL/NHLBI NIH HHS/United States
- S10 OD023469/OD/NIH HHS/United States
- R35 HL161185/HL/NHLBI NIH HHS/United States
- P30 CA125123/CA/NCI NIH HHS/United States
- K01 DE026561/DE/NIDCR NIH HHS/United States
- R50 CA243707/CA/NCI NIH HHS/United States
- F31 HL156681/HL/NHLBI NIH HHS/United States
- R01 HL130804/HL/NHLBI NIH HHS/United States
- S10 RR024574/RR/NCRR NIH HHS/United States
- F30 HL145908/HL/NHLBI NIH HHS/United States
- R01 HL148785/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
