

Economic Evaluation of Using Daily Prednisolone versus Placebo at the Time of an Upper Respiratory Tract Infection for the Management of Children with Steroid-Sensitive Nephrotic Syndrome: A Model-Based Analysis
- PMID: 35733076
- PMCID: PMC9283622
- DOI: 10.1007/s41669-022-00334-6
Economic Evaluation of Using Daily Prednisolone versus Placebo at the Time of an Upper Respiratory Tract Infection for the Management of Children with Steroid-Sensitive Nephrotic Syndrome: A Model-Based Analysis
Abstract
Background: Childhood steroid-sensitive nephrotic syndrome is a frequently relapsing disease with significant short- and long-term complications, leading to high healthcare costs and reduced quality of life for patients. The majority of relapses are triggered by upper respiratory tract infections (URTIs) and evidence shows that daily low-dose prednisolone at the time of infection may reduce the risk of relapse.
Objective: The aim of this study was to assess the cost effectiveness of a 6-day course of low-dose prednisolone at the start of a URTI when compared with placebo.
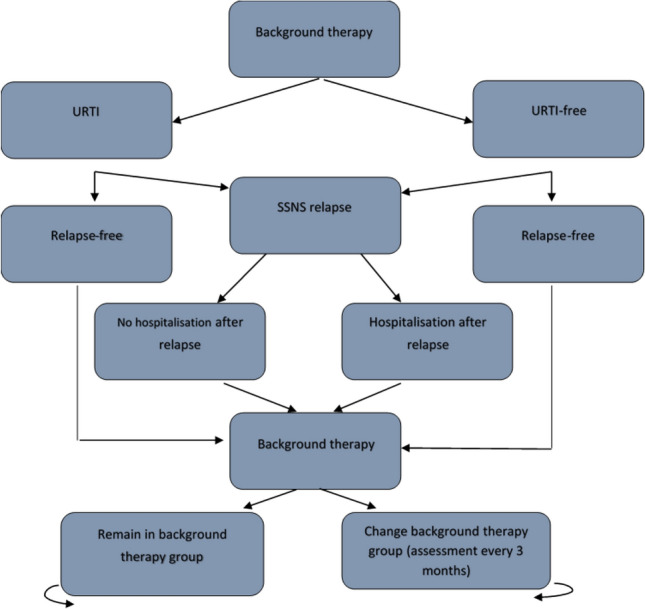
Methods: A state-transition Markov model was developed to conduct a cost-utility analysis with the outcome measured in quality-adjusted life-years (QALYs). Resource use and outcome data were derived from the PREDNOS2 trial. The analysis was performed from a UK National Health Service perspective and the results were extrapolated to adulthood. Model parameter and structural uncertainty were assessed using sensitivity analyses.
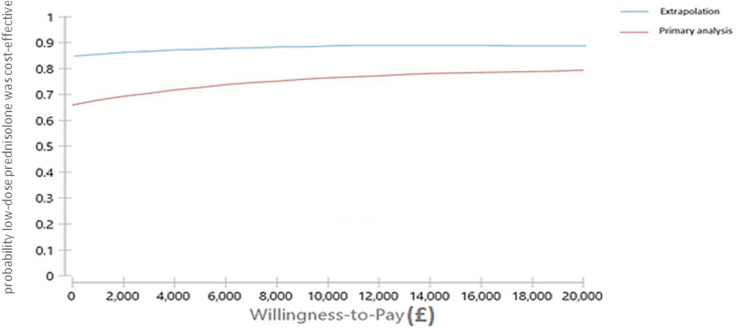
Results: The base-case results showed that administering low-dose prednisolone at the time of a URTI generated more QALYs and a lower mean cost at 1 year compared with placebo. In the long-term, low-dose prednisolone was associated with a cost saving (£176) and increased effectiveness (0.01 QALYs) compared with placebo and thus remained the dominant treatment option. These findings were robust to all sensitivity analyses.
Conclusion: A 6-day course of low-dose prednisolone at the time of a URTI in children with steroid-sensitive nephrotic syndrome has the potential to reduce healthcare costs and improve quality of life compared with placebo.
© 2022. The Author(s).
Conflict of interest statement
Martin T. Christian reported serving as a member of the Clinical Practice Guideline Group for Steroid Sensitive Nephrotic Syndrome of the International Pediatric Nephrology Association during the conduct of this study. Nicholas J.A. Webb reported being an employee of Novartis since August 2018 outside the submitted work. Nafsika Afentou reported receiving grants from the National Institute for Health Research (NIHR) outside the submitted work. Emma Frew reported receiving grants from the NIHR and Zhejiang Yongning Pharmaceutical Co. Ltd outside the submitted work. Elizabeth A. Brettell reported receiving grants from the NIHR during the conduct of this study. David V. Milford reported receiving grants from the NIHR during the conduct of this study. Natalie J. Ives reported receiving grants from the NIHR during the conduct of this study. Samir Mehta, Rebecca L. Woolley, Adam R. Khan, Detlef Bockenhauer, Moin A. Saleem, Angela S. Hall, Ania Koziell, Heather Maxwell, Shivaram Hegde, Hitesh Prajapati, Rodney D. Gilbert, Caroline Jones, Karl McKeever, and Wendy Cook have no conflicts of interest to declare.
Figures

References
-
- Rees L, et al. Paediatric Nephrology (Oxford Specialist Handbooks in Paediatrics) Oxford: Oxford University Press; 2012.
LinkOut - more resources
Full Text Sources
