

Risk factor analysis of postoperative pancreatic fistula after distal pancreatectomy, with a focus on pancreas-visceral fat CT value ratio and serrated pancreatic contour
- PMID: 35733145
- PMCID: PMC9215066
- DOI: 10.1186/s12893-022-01650-8
Risk factor analysis of postoperative pancreatic fistula after distal pancreatectomy, with a focus on pancreas-visceral fat CT value ratio and serrated pancreatic contour
Abstract
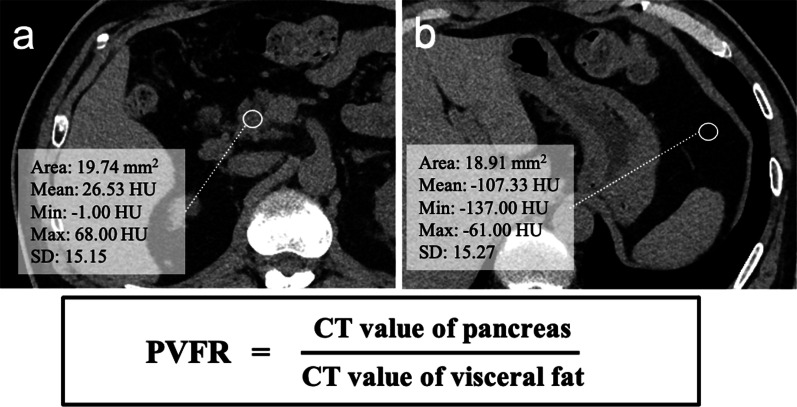
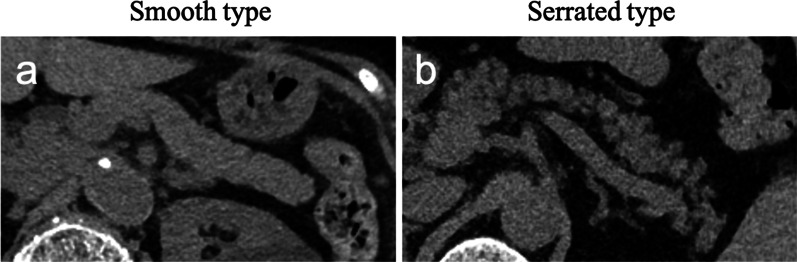
Background: In pancreaticoduodenectomy, the pancreas-visceral fat CT value ratio and serrated pancreatic contour on preoperative CT have been revealed as risk factors for postoperative pancreatic fistulas. We aimed to evaluate whether they could also serve as risk factors for postoperative pancreatic fistulas after distal pancreatectomy.
Methods: A total of 251 patients that underwent distal pancreatectomy at our department from 2006 to 2020 were enrolled for the study. We retrospectively analyzed risk factors for postoperative pancreatic fistulas after distal pancreatectomy using various pre and intraoperative factors, including preoperative CT findings, such as pancreas-visceral fat CT value ratio and serrated pancreatic contour.
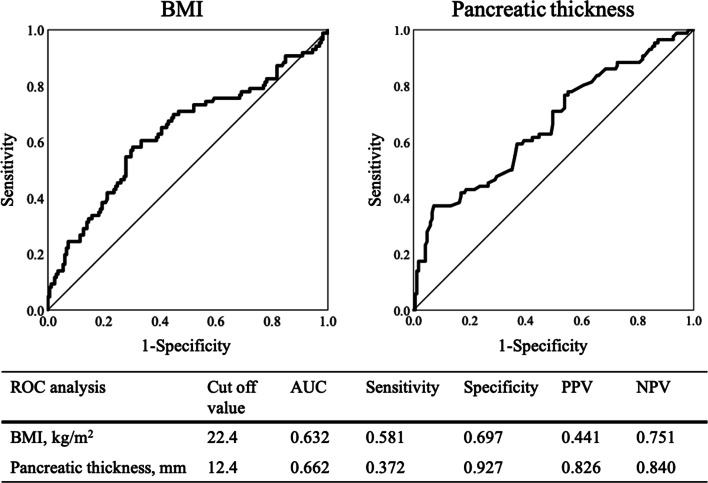
Results: The study population included 147 male and 104 female participants (median age, 68 years; median body mass index, 21.4 kg/m2), including 64 patients with diabetes mellitus (25.5%). Preoperative CT evaluation showed a serrated pancreatic contour in 80 patients (31.9%), a pancreatic thickness of 9.3 mm (4.0-22.0 mm), pancreatic parenchymal CT value of 41.8 HU (4.3-22.0 HU), and pancreas-visceral fat CT value ratio of - 0.41 (- 4.88 to - 0.04). Postoperative pancreatic fistulas were developed in 34.2% of the patients. Univariate analysis of risk factors for postoperative pancreatic fistulas showed that younger age (P = 0.005), high body mass index (P = 0.001), absence of diabetes mellitus (P = 0.002), high preoperative C-reactive protein level (P = 0.024), pancreatic thickness (P < 0.001), and high pancreatic parenchymal CT value (P = 0.018) were significant risk factors; however, pancreas-visceral fat CT value ratio (P = 0.337) and a serrated pancreatic contour (P = 0.122) did not serve as risk factors. Multivariate analysis showed that high body mass index (P = 0.032), absence of diabetes mellitus (P = 0.001), and pancreatic thickness (P < 0.001) were independent risk factors.
Conclusion: The pancreas-visceral fat CT value ratio and serrated pancreatic contour evaluated using preoperative CT were not risk factors for postoperative pancreatic fistulas after distal pancreatectomy. High body mass index, absence of diabetes mellitus, and pancreatic thickness were independent risk factors, and a close-to-normal pancreas with minimal fat deposition or atrophy is thought to indicate a higher risk of postoperative pancreatic fistulas after distal pancreatectomy.
Keywords: CT value; Diabetes mellitus; Distal pancreatectomy; Postoperative pancreatic fistula; Serrated pancreas; Visceral fat.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Pancreas-visceral fat CT value ratio and serrated pancreatic contour are strong predictors of postoperative pancreatic fistula after pancreaticojejunostomy.BMC Surg. 2020 Jun 11;20(1):129. doi: 10.1186/s12893-020-00785-w. BMC Surg. 2020. PMID: 32527310 Free PMC article.
-
Pancreatic Fat and Body Composition Measurements by Computed Tomography are Associated with Pancreatic Fistula After Pancreatectomy.Ann Surg Oncol. 2021 Jan;28(1):530-538. doi: 10.1245/s10434-020-08581-9. Epub 2020 May 20. Ann Surg Oncol. 2021. PMID: 32436185
-
Preoperative CT scan helps to predict the occurrence of severe pancreatic fistula after pancreaticoduodenectomy.Ann Surg. 2012 Jul;256(1):139-45. doi: 10.1097/SLA.0b013e318256c32c. Ann Surg. 2012. PMID: 22609844
-
Effect of artificial or autologous coverage of the pancreatic remnant or anastomosis on postoperative pancreatic fistulas after partial pancreatectomy: meta-analysis of randomized clinical trials.BJS Open. 2024 May 8;8(3):zrae059. doi: 10.1093/bjsopen/zrae059. BJS Open. 2024. PMID: 38814751 Free PMC article.
-
"Mitigation strategies for post-operative pancreatic fistula after pancreaticoduodenectomy in high-risk pancreas: an evidence-based algorithmic approach"-a narrative review.Chin Clin Oncol. 2022 Feb;11(1):6. doi: 10.21037/cco-22-6. Chin Clin Oncol. 2022. PMID: 35255695 Review.
Cited by
-
Simple Preoperative Imaging Measurements Predict Postoperative Pancreatic Fistula After Pancreatoduodenectomy.Ann Surg Oncol. 2024 Mar;31(3):1898-1905. doi: 10.1245/s10434-023-14564-3. Epub 2023 Nov 15. Ann Surg Oncol. 2024. PMID: 37968411 Free PMC article.
-
Quantitative edge analysis of pancreatic margins in patients with head pancreatic tumors: correlations between pancreatic margins and the onset of postoperative pancreatic fistula.Eur Radiol. 2024 Mar;34(3):1515-1523. doi: 10.1007/s00330-023-10200-6. Epub 2023 Sep 2. Eur Radiol. 2024. PMID: 37658898
-
Correlation Between Fatty Pancreas Disease and Pancreatic Diseases, Perioperative Complications of Pancreatic Surgery.Cancer Manag Res. 2025 Mar 29;17:723-730. doi: 10.2147/CMAR.S508567. eCollection 2025. Cancer Manag Res. 2025. PMID: 40177416 Free PMC article. Review.
References
-
- Kawai M, Hirono S, Okada K, Sho M, Nakajima Y, Eguchi H, et al. Randomized controlled trial of pancreaticojejunostomy versus stapler closure of the pancreatic stump during distal pancreatectomy to reduce pancreatic fistula. Ann Surg. 2016;264:180–187. doi: 10.1097/SLA.0000000000001395. - DOI - PMC - PubMed
-
- Chong E, Ratnayake B, Lee S, French JJ, Wilson C, Roberts KJ, et al. Systematic review and meta-analysis of risk factors of postoperative pancreatic fistula after distal pancreatectomy in the era of 2016 International Study Group pancreatic fistula definition. HPB (Oxford) 2021;23:1139–1151. doi: 10.1016/j.hpb.2021.02.015. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
