

Long-term outcomes after extra-levator versus conventional abdominoperineal excision for low rectal cancer
- PMID: 35733206
- PMCID: PMC9219120
- DOI: 10.1186/s12893-022-01692-y
Long-term outcomes after extra-levator versus conventional abdominoperineal excision for low rectal cancer
Abstract
Purpose: Extralevator (ELAPE) and abdominoperineal excision (APE) are two major surgical approaches for low rectal cancer patients. Although excellent short-term efficacy is achieved in patients undergoing ELAPE, the long-term benefits have not been established. In this study we evaluated the safety, pathological and survival outcomes in rectal cancer patients who underwent ELAPE and APE.
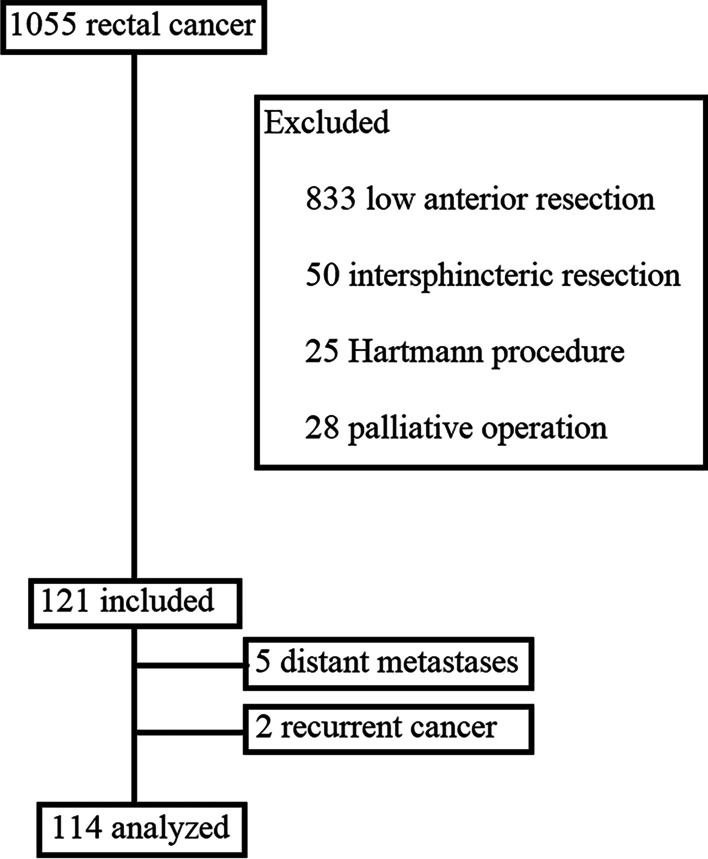
Methods: One hundred fourteen patients were enrolled, including 68 in the ELAPE group and 46 in the APE group at the Beijing Chaoyang Hospital, Capital Medical University from January 2011 to November 2020. The baseline characteristics, overall survival (OS), progression-free survival (PFS), and local recurrence-free survival (LRFS) were calculated and compared between the two groups.
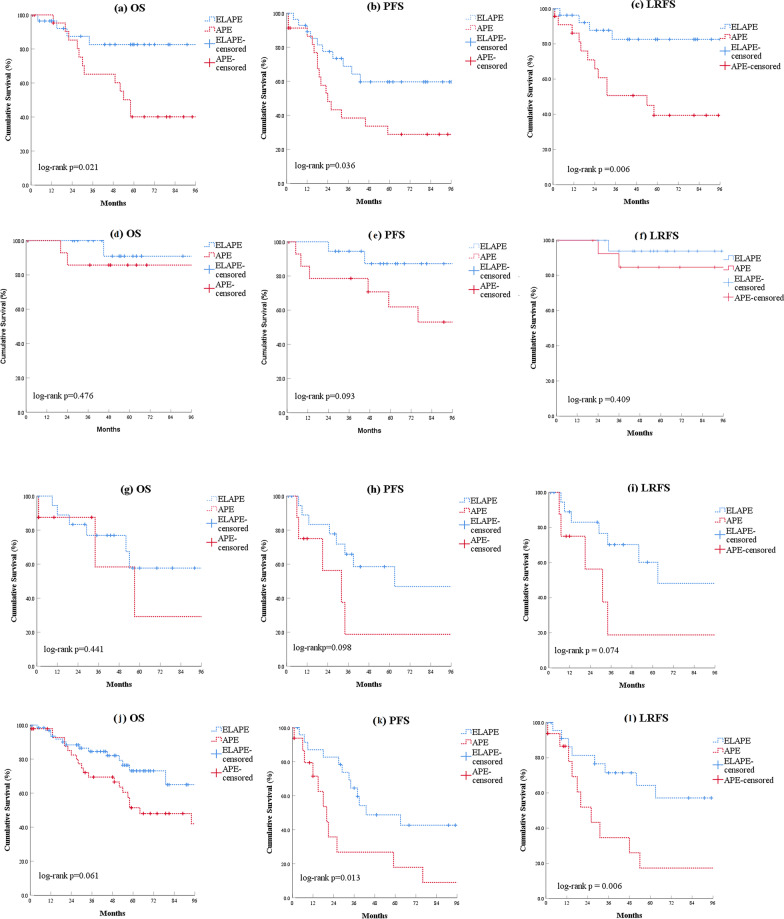
Results: Demographics and tumor stage were comparable between the two groups. The 5-year PFS (67.2% versus 38.6%, log-rank P = 0.008) were significantly improved in the ELAPE group compared to the APE group, and the survival advantage was especially reflected in patients with pT3 tumors, positive lymph nodes or even those who have not received neoadjuvant chemoradiotherapy. Multivariate analysis showed that APE was an independent risk factor for OS (hazard ratio 3.000, 95% confidence interval 1.171 to 4.970, P = 0.004) and PFS (hazard ratio 2.730, 95% confidence interval 1.506 to 4.984, P = 0.001).
Conclusion: Compared with APE, ELAPE improved long-term outcomes for low rectal cancer patients, especially among patients with pT3 tumors, positive lymph nodes or those without neoadjuvant chemoradiotherapy.
Keywords: Abdominoperineal excision; Extralevator abdominoperineal excision; Rectal cancer; Suvival.
© 2022. The Author(s).
Conflict of interest statement
The authors of the article do not have commercial associations (e.g., consultancies, stock ownership, equity interests, patent-licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Figures


Similar articles
-
Multicenter study of surgical and oncologic outcomes of extra-levator versus conventional abdominoperineal excision for lower rectal cancer.Eur J Surg Oncol. 2020 Jan;46(1):115-122. doi: 10.1016/j.ejso.2019.08.017. Epub 2019 Aug 21. Eur J Surg Oncol. 2020. PMID: 31471089
-
Long-term outcome of extralevator abdominoperineal excision (ELAPE) for low rectal cancer.Int J Colorectal Dis. 2016 Oct;31(10):1729-37. doi: 10.1007/s00384-016-2637-z. Epub 2016 Sep 9. Int J Colorectal Dis. 2016. PMID: 27631643
-
Extralevator versus standard abdominoperineal excision in locally advanced rectal cancer: a retrospective study with long-term follow-up.Int J Colorectal Dis. 2018 Apr;33(4):375-381. doi: 10.1007/s00384-018-2977-y. Epub 2018 Feb 14. Int J Colorectal Dis. 2018. PMID: 29445870
-
Extralevator abdominoperineal excision for advanced low rectal cancer: Where to go.World J Gastroenterol. 2020 Jun 14;26(22):3012-3023. doi: 10.3748/wjg.v26.i22.3012. World J Gastroenterol. 2020. PMID: 32587445 Free PMC article. Review.
-
Short-term outcome of extra-levator abdominoperineal excision for rectal cancer.Int J Colorectal Dis. 2011 Jul;26(7):919-25. doi: 10.1007/s00384-011-1157-0. Epub 2011 Feb 25. Int J Colorectal Dis. 2011. PMID: 21350936 Review.
Cited by
-
Laparoscopic extralevator abdominoperineal excision in distal rectal cancer patients: a retrospective comparative study.BMC Surg. 2022 Dec 8;22(1):418. doi: 10.1186/s12893-022-01865-9. BMC Surg. 2022. PMID: 36482294 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
