

Feasibility of Extracting Meaningful Patient Centered Outcomes From the Electronic Health Record Following Critical Illness in the Elderly
- PMID: 35733861
- PMCID: PMC9207323
- DOI: 10.3389/fmed.2022.826169
Feasibility of Extracting Meaningful Patient Centered Outcomes From the Electronic Health Record Following Critical Illness in the Elderly
Abstract
Background: Meaningful patient centered outcomes of critical illness such as functional status, cognition and mental health are studied using validated measurement tools that may often be impractical outside the research setting. The Electronic health record (EHR) contains a plethora of information pertaining to these domains. We sought to determine how feasible and reliable it is to assess meaningful patient centered outcomes from the EHR.
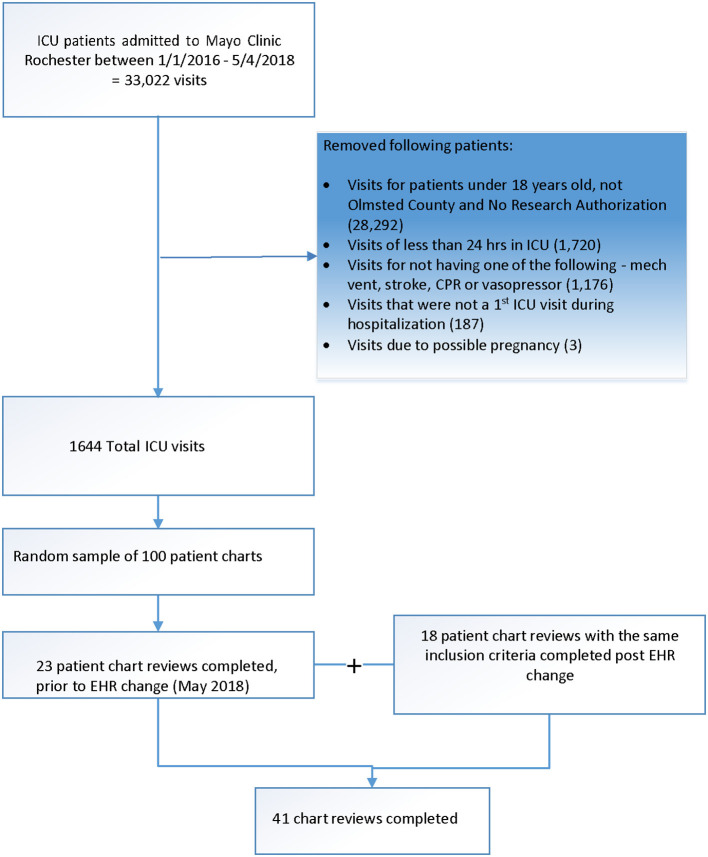
Methods: Two independent investigators reviewed EHR of a random sample of ICU patients looking at documented assessments of trajectory of functional status, cognition, and mental health. Cohen's kappa was used to measure agreement between 2 reviewers. Post ICU health in these domains 12 month after admission was compared to pre- ICU health in the 12 months prior to assess qualitatively whether a patient's condition was "better," "unchanged" or "worse." Days alive and out of hospital/health care facility was a secondary outcome.
Results: Thirty six of the 41 randomly selected patients (88%) survived critical illness. EHR contained sufficient information to determine the difference in health status before and after critical illness in most survivors (86%). Decline in functional status (36%), cognition (11%), and mental health (11%) following ICU admission was observed compared to premorbid baseline. Agreement between reviewers was excellent (kappa ranging from 0.966 to 1). Eighteen patients (44%) remained home after discharge from hospital and rehabilitation during the 12- month follow up.
Conclusion: We demonstrated the feasibility and reliability of assessing the trajectory of changes in functional status, cognition, and selected mental health outcomes from EHR of critically ill patients. If validated in a larger, representative sample, these outcomes could be used alongside survival in quality improvement studies and pragmatic clinical trials.
Keywords: critical illness; days alive and out of hospital/health care facility (DAOH); electronic health records (EHR); patient important outcomes; trajectory.
Copyright © 2022 Ahmad, Tarabochia, Budahn, Lemahieu, Anderson, Vashistha, Karnatovskaia and Gajic.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Determining Goal Concordant Care in the Intensive Care Unit Using Electronic Health Records.J Pain Symptom Manage. 2023 Mar;65(3):e199-e205. doi: 10.1016/j.jpainsymman.2022.11.002. Epub 2022 Nov 17. J Pain Symptom Manage. 2023. PMID: 36400406 Free PMC article.
-
Adult patient access to electronic health records.Cochrane Database Syst Rev. 2021 Feb 26;2(2):CD012707. doi: 10.1002/14651858.CD012707.pub2. Cochrane Database Syst Rev. 2021. PMID: 33634854 Free PMC article.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
-
Functional status after critical illness: agreement between patient and proxy assessments.Age Ageing. 2015 May;44(3):506-10. doi: 10.1093/ageing/afu163. Epub 2014 Oct 16. Age Ageing. 2015. PMID: 25324334 Free PMC article.
-
Effect of Systematic Intensive Care Unit Triage on Long-term Mortality Among Critically Ill Elderly Patients in France: A Randomized Clinical Trial.JAMA. 2017 Oct 17;318(15):1450-1459. doi: 10.1001/jama.2017.13889. JAMA. 2017. PMID: 28973065 Free PMC article. Clinical Trial.
Cited by
-
Determining Goal Concordant Care in the Intensive Care Unit Using Electronic Health Records.J Pain Symptom Manage. 2023 Mar;65(3):e199-e205. doi: 10.1016/j.jpainsymman.2022.11.002. Epub 2022 Nov 17. J Pain Symptom Manage. 2023. PMID: 36400406 Free PMC article.
-
Scoping review exploring the impact of hip fracture in older adults with cognitive impairment or dementia.BMJ Open. 2025 Apr 27;15(4):e093893. doi: 10.1136/bmjopen-2024-093893. BMJ Open. 2025. PMID: 40288797 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources