

Tension-band Plating for Leg-length Discrepancy Correction
- PMID: 35734032
- PMCID: PMC9166256
- DOI: 10.5005/jp-journals-10080-1547
Tension-band Plating for Leg-length Discrepancy Correction
Abstract
Aim: Dual tension-band plates are used for temporary epiphysiodesis and longitudinal guided growth. The study aim was to assess rate of correction, to identify development of femoral and tibial intra-articular deformity during correction and to document resumption of growth after plate removal.
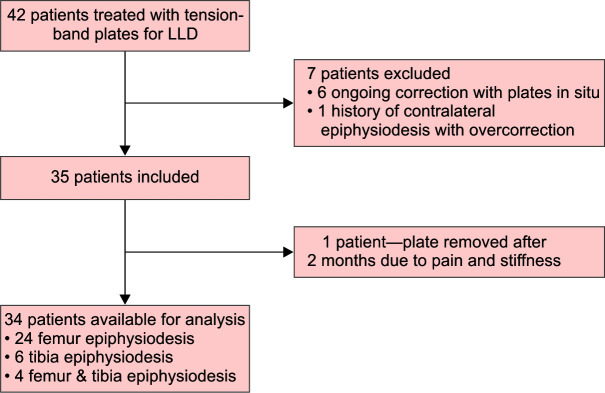
Materials and methods: A retrospective study of 34 consecutive patients treated with dual tension-band plates between 2012 and 2020 was performed. Twenty-four patients had surgery at the distal femur, six at the proximal tibia and four at both. Twenty-five female patients were treated at a mean age of 11.6 (±1.4) years and nine male patients at 13.5 (±1.5) years. Measurements were performed on standardised long-leg radiographs and included leg-length discrepancy (LLD), joint line congruency angle (JLCA), tibial roof angle, femoral floor angle and notch-intercondylar distance. Measurements were taken pre-operatively, at the end of discrepancy correction and at skeletal maturity.
Results: The LLD reduced by a mean of 12.9 mm (95% CI 10.2-15.5) with the mean residual difference 8.4 mm (95% CI 5.4-11.4). The mean correction rate for the proximal tibia was 0.40 (SD 0.33) mm/month and 0.68 (SD 0.36) mm/month for the distal femur. A significant mean change in residual LLD [-2.5 mm (95% CI -4.2 to -0.7)] was observed between plate removal and skeletal maturity at the femoral level only. After length discrepancy correction, the tibial roof angle showed a significant difference of 8.4° (95% CI 13.4-3.4) between legs. In femoral epiphysiodesis patients, no important differences were observed.
Conclusion: A significant reduction in LLD can be achieved using dual tension-band plating. A change in intra-articular morphology was observed only in the proximal tibia and not in the distal femur. In the authors' opinion, tension-band plating is a useful tool for leg-length equalisation but should be reserved for younger patients or when residual growth is difficult to predict. It is one of the management strategies for limb-length difference prior to skeletal maturity.
How to cite this article: Tolk JJ, Merchant R, Calder PR, et al. Tension-band Plating for Leg-length Discrepancy Correction. Strategies Trauma Limb Reconstr 2022;17(1):19-25.
Keywords: Epiphysiodesis; Guided growth; Leg-length discrepancy; Tension-band plating.
Copyright © 2022; The Author(s).
Conflict of interest statement
Source of support: Nil Conflict of interest: None
Figures



References
LinkOut - more resources
Full Text Sources
Research Materials
