

This is a preprint.
It has not yet been peer reviewed by a journal.
The National Library of Medicine is
running a pilot
to include preprints that result from research funded by NIH in PMC and PubMed.
[Preprint]. 2022 Jun 17:2022.06.16.22276392.
doi: 10.1101/2022.06.16.22276392.
COVID-19 redux: clinical, virologic, and immunologic evaluation of clinical rebound after nirmatrelvir/ritonavir
Affiliations
- PMID: 35734093
- PMCID: PMC9216730
- DOI: 10.1101/2022.06.16.22276392
Item in Clipboard
COVID-19 redux: clinical, virologic, and immunologic evaluation of clinical rebound after nirmatrelvir/ritonavir
medRxiv.
.
Update in
-
Clinical, Virologic, and Immunologic Evaluation of Symptomatic Coronavirus Disease 2019 Rebound Following Nirmatrelvir/Ritonavir Treatment.Clin Infect Dis. 2023 Feb 18;76(4):573-581. doi: 10.1093/cid/ciac663. Clin Infect Dis. 2023. PMID: 36200701 Free PMC article.
Abstract
Clinical rebound of COVID-19 after nirmatrelvir/ritonavir treatment has been reported. We performed clinical, virologic, and immune measurements in seven patients with symptomatic rebound, six after nirmatrelvir/ritonavir treatment and one without previous treatment. There was no evidence of severe disease or impaired antibody and T-cell responses in people with rebound symptoms.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures
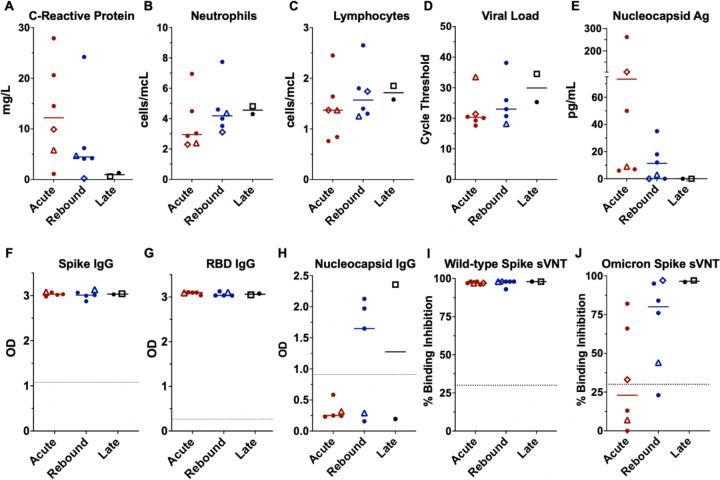
Lines represent median and points represent individual results. The two longitudinal patients are identified by an open diamond (patient 1) and open triangle (patient 2), respectively. The open square represents the COVID-19 rebound patient that did not receive NMV-r. Clinical values for C-reactive protein, absolute neutrophil count, and absolute lymphocyte count across the acute (red), rebound (blue), and late presenting (black) COVID-19 cohorts (A, B, C). SARS-CoV-2 cycle threshold from nasal swab samples (D) and serum nucleocapsid antigen (E). Antibody levels by enzyme-linked immunosorbent assay (ELISA) against the spike protein, spike - receptor binding domain (RBD), and the nucleocapsid protein (F, G, H) presented as optical density (OD). ELISA data not available for longitudinal patient-1 (diamond). Surrogate viral neutralization test (sVNT) to detect neutralizing antibodies against the wild-type (I) and Omicron (J) spike protein presented as percent binding inhibition. Dotted lines represent the cut-off for a positive result for the antibody tests (F-J). Abbreviations: Ag – antigen, OD – optical density, RBD – receptor-binding domain, sVNT – surrogate viral neutralization test.
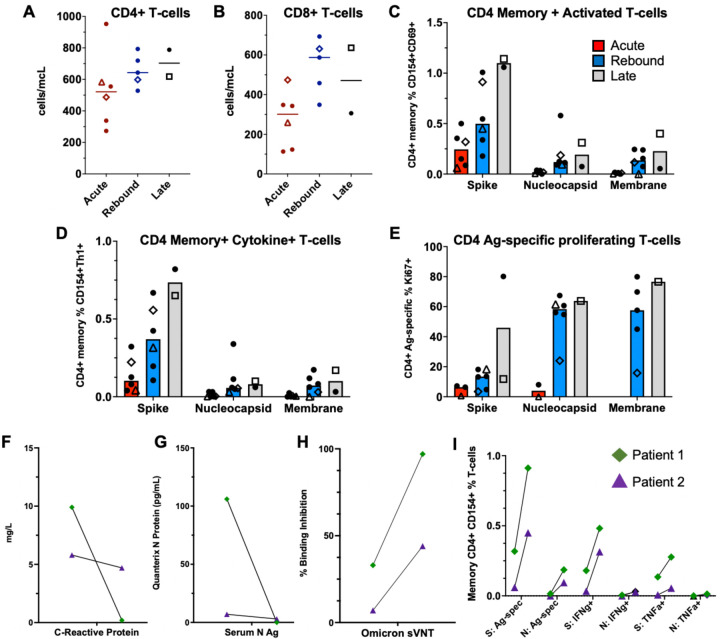
Absolute T-cell counts compared across groups (A-B). Lines represent median values and points represent individual results. The two-longitudinal patients are identified by an open triangle and open diamond. The empty square represents the COVID-19 rebound patient that did not receive NMV-r. T-cell counts not available for longitudinal patient-2 (triangle) at rebound timepoint. T-cell stimulations were performed with peptide pools corresponding to spike, nucleocapsid, and membrane proteins as listed on the x-axis. Bars represent medians and groups are defined as acute (red), rebound (blue), and late presentations (gray). SARS-CoV-2 specific CD4 T-cell responses are highlighted by memory, cytokine-producing (CD154+IFNγ+, CD154+TNFα+ or CD154+IL-2+), activated (CD154+CD69+), or antigen-specific proliferating T-cells (Ki67+) (C-E). For phenotyping of Ki67+ cells, a threshold of at least 20-events and a 2-fold increase over unstimulated cells was used, and samples were excluded if they did not meet these thresholds (E). Serum nucleocapsid antigen (Ag) and C-reactive protein trends from the two longitudinal patients (F-G). T-cell responses and neutralizing antibodies from the acute and rebound presentation for two patients with longitudinal samples (H-I). T-cell responses are from spike (S) and nucleocapsid (N) stimulations. Antigen-specific CD4 T-cells defined by (CD154+CD69+, CD154+IFNγ+ and CD154+TNFα+), and neutralizing antibodies represented by percent binding inhibition on the surrogate virus neutralization test (sVNT). Abbreviations: Ag – antigen, S – spike, N – nucleocapsid, Ag-spec – antigen-specific, sVNT - surrogate virus neutralization test, N Ag – nucleocapsid antigen.
References
-
- Emergency Use Authorization (EUA) for Paxlovid (nirmatrelvir tablets co-packaged with ritonavir tablets) Center for Drug Evaluation and Research (CDER) Review. In: Center for Drug Evaluation and Research (CDER); 2021.
-
- Charness M, Gupta K, Stack G, et al. Rapid Relapse of Symptomatic Omicron SARS-CoV-2 Infection Following Early Suppression with Nirmatrelvir/Ritonavir. medRxiv Preprint. 2022.
-
- Gupta K, Strymish J, Stack G, Charness M. Rapid Relapse of Symptomatic SARS-CoV-2 Infection Following Early Suppression with Nirmatrelvir/Ritonavir. medRxiv Preprint. 2022.
Publication types
LinkOut - more resources
Full Text Sources