

Late-Onset Hereditary Transthyretin Amyloidosis Val30Met in an Elderly Person in a Non-Endemic Area
- PMID: 35734096
- PMCID: PMC9208636
- DOI: 10.2147/IMCRJ.S357236
Late-Onset Hereditary Transthyretin Amyloidosis Val30Met in an Elderly Person in a Non-Endemic Area
Abstract
Introduction: Patients with late-onset transthyretin Val30Met-associated hereditary transthyretin amyloidosis (hATTR) in non-endemic areas still remain undiagnosed because of diverse clinical presentations and various non-specific symptoms.
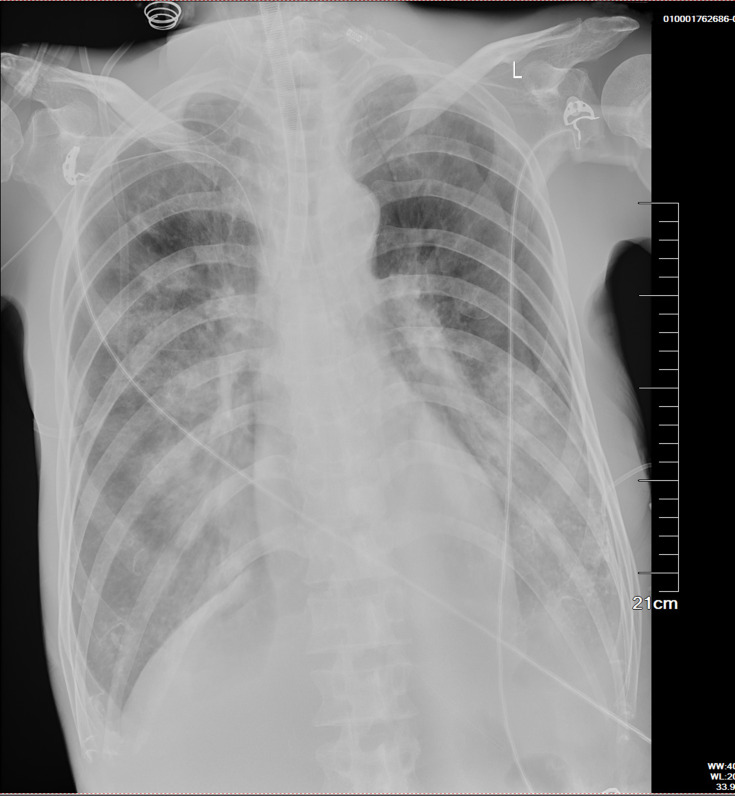
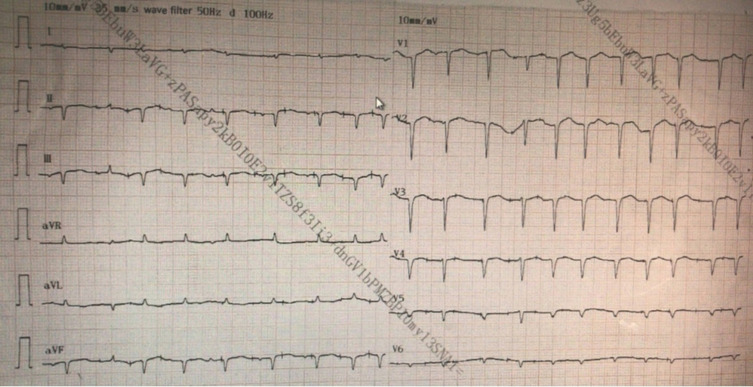
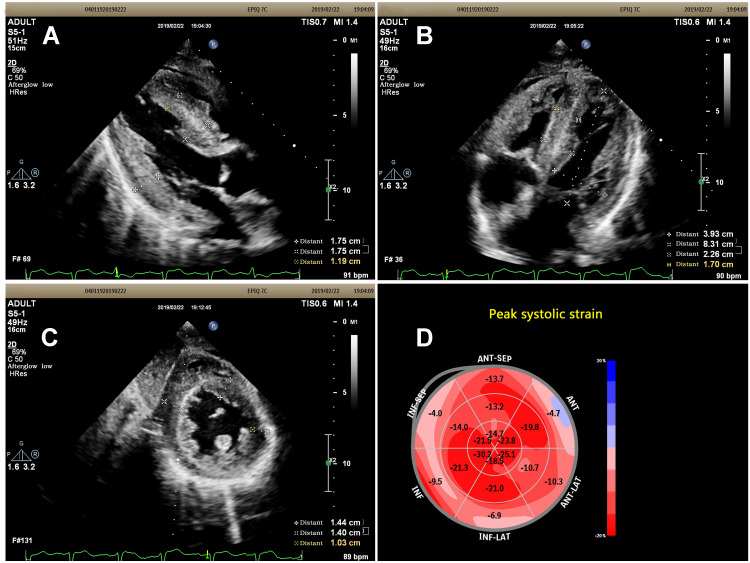
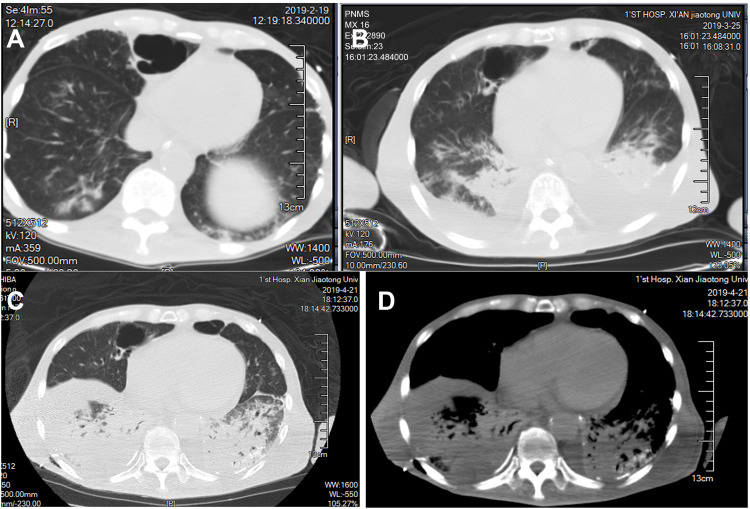
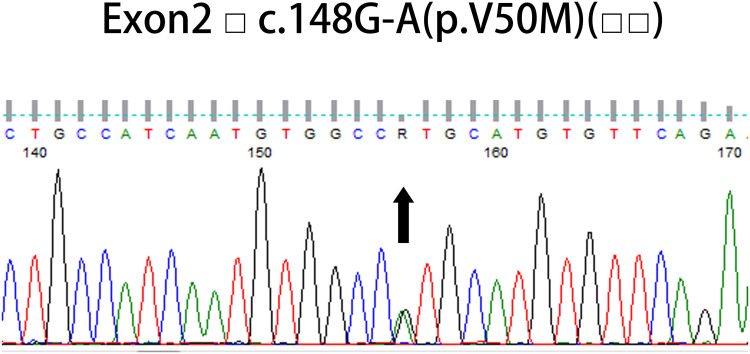
Case presentation: A 76-year-old male patient presented with progressive numbness, pain and weakness in his limbs, sweating, constipation and unexplained weight loss over the past seven years. He has shortness of breath, edema and hypotension for one month. The low QRS voltage on limb leads was not consistent with left ventricular hypertrophy, which is an important clue of cardiac amyloidosis (CA). The results of echocardiography speckle tracking imaging were consistent with CA. Serum immunofixation electrophoresis was negative, and serum-free light chain Fκ/Fλ ratio is normal or close to normal (0.26-1.65) for the patient, so AL amyloidosis can be excluded. A missense mutation c. 148 G-A Val30Met (p.Val50Met) was detected in TTR gene sequencing. The genetic finding confirmed hATTR Val30Met, familial amyloid polyneuropathy (FAP) and CA for the patient. The treatment effect was poor, and he died of cardiac involvement.
Conclusion: It is challenge to make early diagnosis in patients with hATTR, due to the diversity of symptoms. Echocardiography is a vital tool in initial diagnosis. Genetic testing played vital roles in the definitive diagnosis of this disease. Raising awareness is critical for early diagnosis and provides opportunities for early treatment.
Keywords: cardiac amyloidosis; familial amyloid polyneuropathy; hereditary transthyretin amyloidosis; speckle tracking imaging.
© 2022 Wang et al.
Conflict of interest statement
Shun Wang and Jing Ping Sun are co-first authors. The authors declare no conflicts of interest in this work.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
