

Relationship between the posterior atrial wall and the esophagus: Esophageal position during atrial fibrillation ablation
- PMID: 35734293
- PMCID: PMC9207737
- DOI: 10.1016/j.hroo.2022.02.007
Relationship between the posterior atrial wall and the esophagus: Esophageal position during atrial fibrillation ablation
Abstract
Background: Atrial fibrillation ablation implies a risk of esophageal thermal injury. Esophageal position can be analyzed with imaging techniques, but evidence for esophageal mobility is inconsistent.
Objectives: The purpose of this study was to analyze esophageal position stability from one procedure to another and during a single procedure.
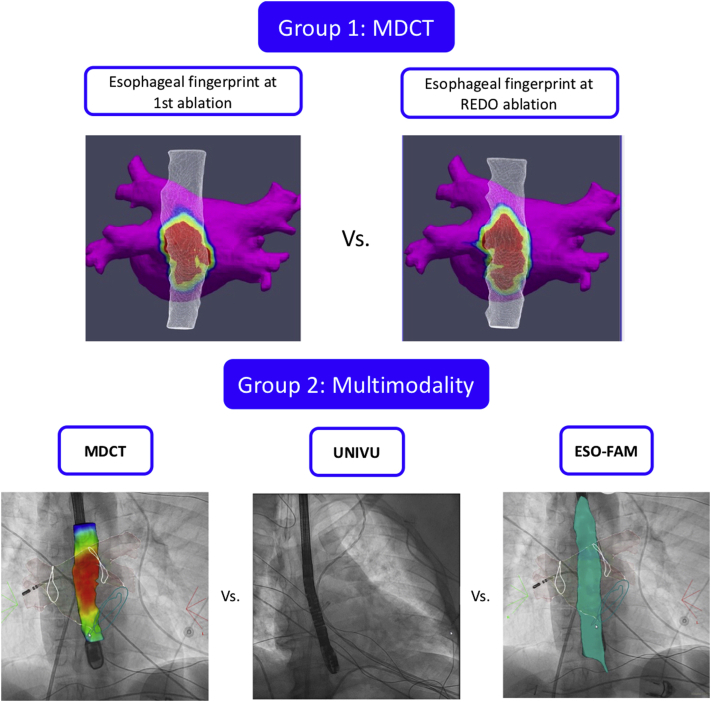
Methods: Esophageal position was compared in 2 patient groups. First, preprocedural multidetector computerized tomography (MDCT) of first pulmonary vein isolation and redo intervention (redo group) was segmented with ADAS 3D™ to compare the stability of the atrioesophageal isodistance prints. Second, 3 imaging modalities were compared for the same procedure (multimodality group): (1) preprocedural MDCT; (2) intraprocedural fluoroscopy obtained with the transesophageal echocardiographic probe in place with CARTOUNIVU™; and (3) esophageal fast anatomic map (FAM) at the end of the procedure. Esophageal position correlation between different imaging techniques was computed in MATLAB using semiautomatic segmentation analysis.
Results: Thirty-five redo patients were analyzed and showed a mean atrioesophageal distance of 1.2 ± 0.6 mm and a correlation between first and redo procedure esophageal fingerprint of 91% ± 5%. Only 3 patients (8%) had a clearly different position. The multi-imaging group was composed of 100 patients. Esophageal position correlation between MDCT and CARTOUNIVU was 82% ± 10%; between MDCT and esophageal FAM was 80% ± 12%; and between esophageal FAM and CARTOUNIVU was 83% ± 15%.
Conclusion: There is high stability of esophageal position between procedures and from the beginning to the end of a procedure. Further research is undergoing to test the clinical utility of the esophageal fingerprinted isodistance map to the posterior atrial wall.
Keywords: Atrial fibrillation; Atrial wall thickness; Atrioesophageal fistula; Catheter ablation; Esophageal position.
© 2022 Published by Elsevier Inc. on behalf of Heart Rhythm Society.
Figures





References
-
- Hindricks G., Potpara T., Dagres N., et al. ESC Scientific Document Group 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373–498. - PubMed
-
- Suenari K., Nakano Y., Hirai Y., et al. Left atrial thickness under the catheter ablation lines in patients with paroxysmal atrial fibrillation: insights from 64-slice multidetector computed tomography. Heart Vessels. 2013;28:360–368. - PubMed
-
- Sanchez-Quintana D., Cabrera J.A., Climent V., Farre J., de Mendonca M.C., Ho S.Y. Anatomic relations between the esophagus and left atrium and relevance for ablation of atrial fibrillation. Circulation. 2005;112:1400–1405. - PubMed
-
- Halbfass P., Pavlov B., Muller P., et al. Progression from esophageal thermal asymptomatic lesion to perforation complicating atrial fibrillation ablation: a single-center registry. Circ Arrhythm Electrophysiol. 2017;10 - PubMed
-
- Lakkireddy D., Reddy Y.M., Atkins D., et al. Effect of atrial fibrillation ablation on gastric motility: the atrial fibrillation gut study. Circ Arrhythm Electrophysiol. 2015;8:531–536. - PubMed
LinkOut - more resources
Full Text Sources
