

Causes and Demographic Factors Affecting Stillbirth in a Tertiary Care Centre in India
- PMID: 35734358
- PMCID: PMC9206988
- DOI: 10.1007/s13224-021-01571-1
Causes and Demographic Factors Affecting Stillbirth in a Tertiary Care Centre in India
Abstract
Introduction: Stillbirth is a global health problem having many emotional, social and economic consequences. India has the largest number of stillbirths per year in the world.
Objective: The objective of this study is to review the causes of stillbirth and classify the causes into maternal, foetal and placental causes and further classify causes by relevant condition at death (ReCoDe) classification. We intend to observe the causes of and demographic factors contributing to the burden of stillbirths. Using this data, the areas of action can be identified and measures can be formulated to reduce a significant number of perinatal mortalities.
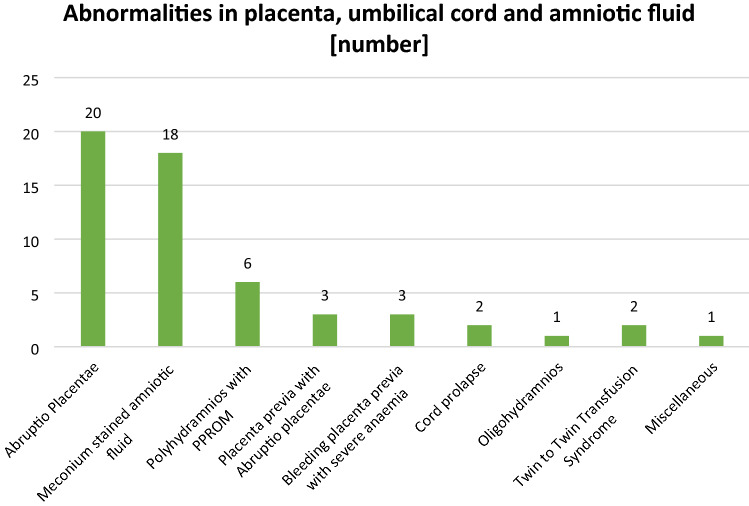
Methodology: This is an observational study of data collected over one year (January 2019-December 2019) from a tertiary care centre in Mumbai, India. The maternal demographic characteristics and causes of stillbirth were studied. The causes of stillbirths were classified into maternal, foetal and placental causes and relevant condition at death (ReCoDe) classification [1].
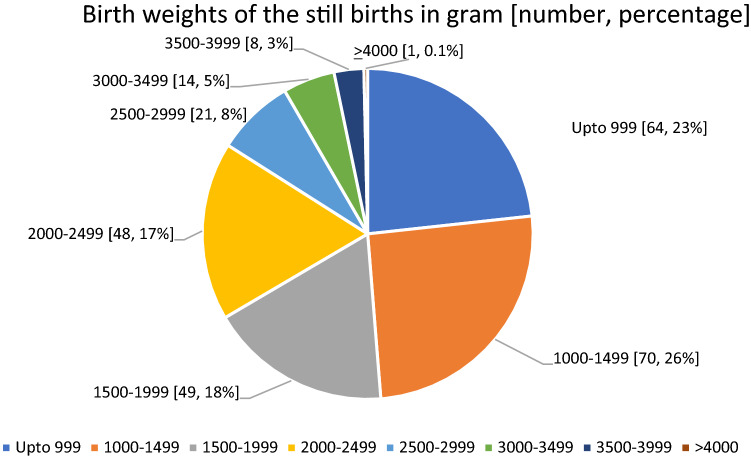
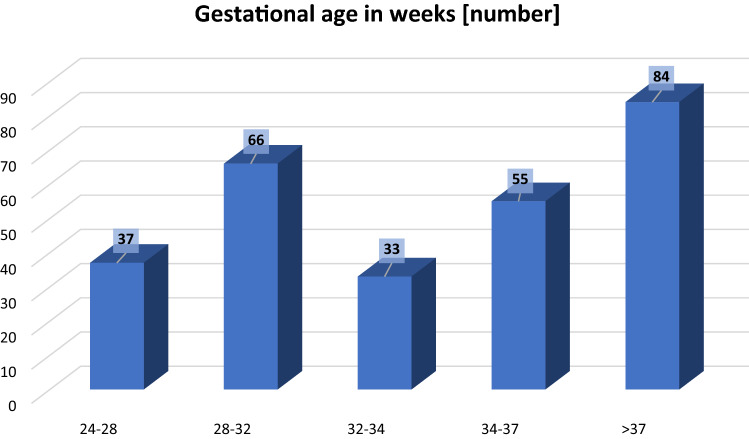
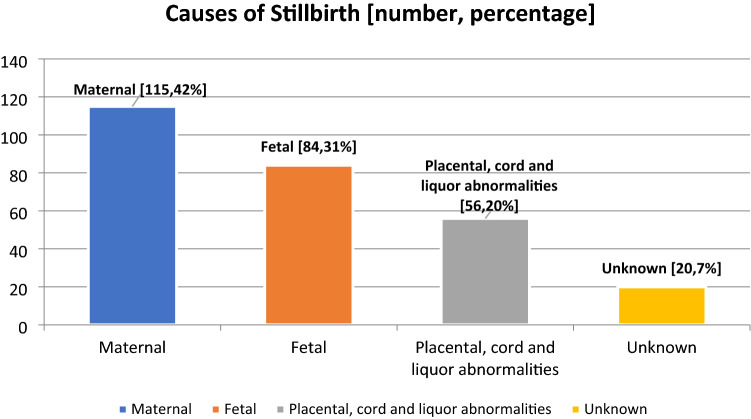
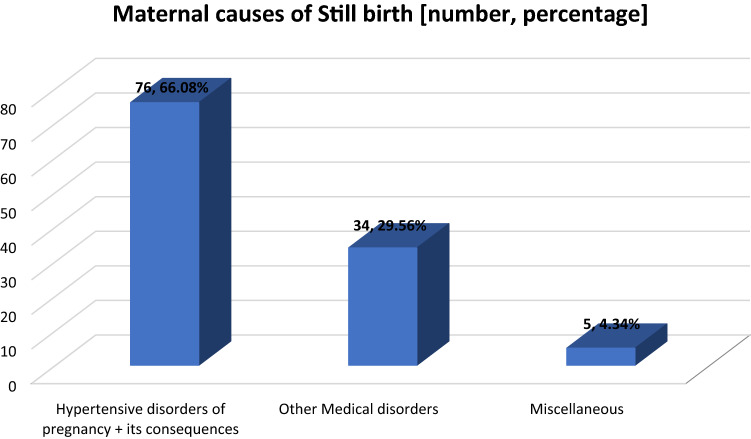
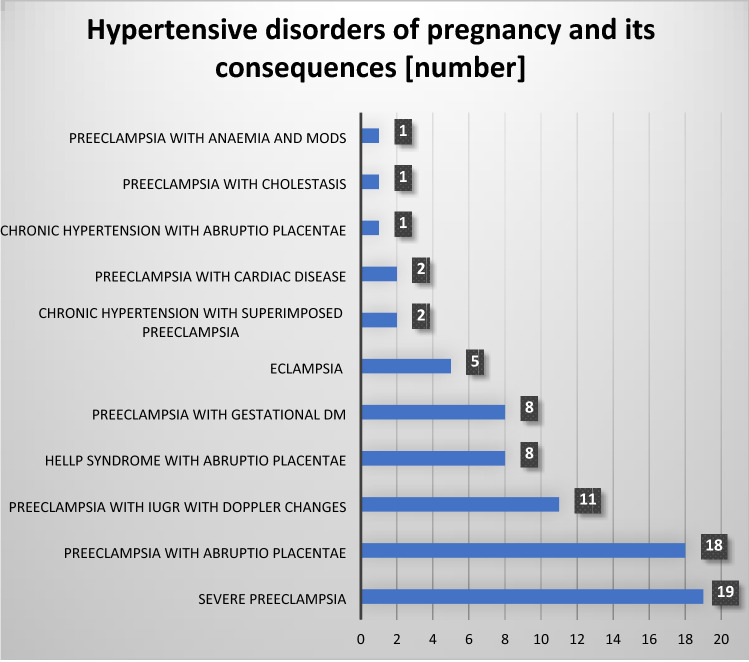
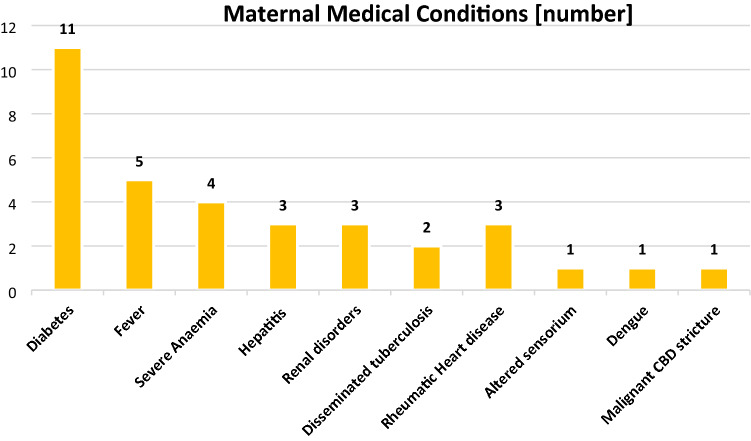
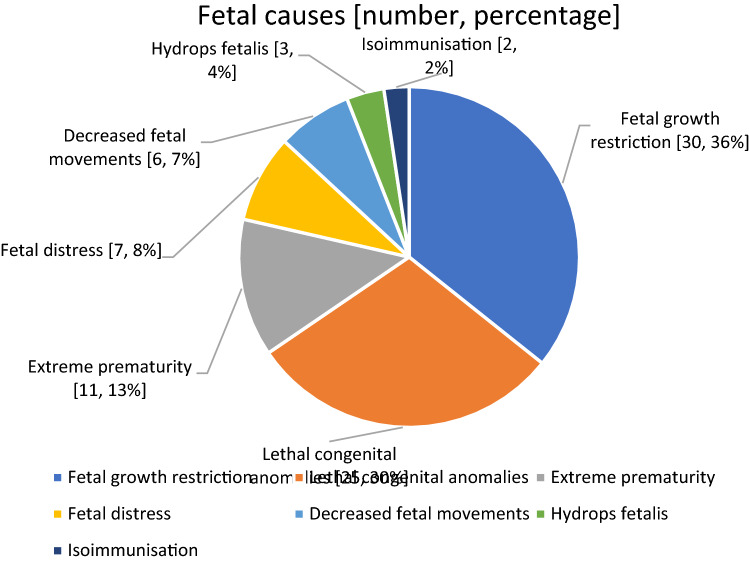
Results: A total of 9074 babies were delivered during this period. There were 275 stillbirths in this year (SBR 30.3 per 1000 total births). Majority of the mothers were in the age group of 26-30 years (32.7%). Almost all the mothers (98.5%) were from urban areas. As per the modified Kuppuswamy classification for urban India, 195 (71.79%) belonged to the upper lower class. 31.2% were primigravidae, and 54.8% had 3 or more antenatal visits. Maternal conditions (pre-eclampsia, diabetes, pre-existing medical disorders) as a group were the cause of maximum number (42%) of stillbirths either directly or as a contributory risk factor. 78% of the stillbirths occurred in the antepartum period. Ours being a referral centre, 65% subjects in the study were referred to us from other peripheral hospitals. 53.8% of the stillborn babies were male. 58.9% were macerated stillbirths. According to the ReCoDe classification, hypertensive disease in pregnancy was the most common cause of stillbirths (76) followed by foetal growth restriction (30).
Conclusion: Most of the stillbirths in this study were due to maternal medical conditions. Out of these conditions, hypertensive disorders of pregnancy and its consequences were the most common (66.08%). Better regulation of the private healthcare sector, provision of healthcare providers and better equipments in peripheral health centres and a well-chalked out referral system will contribute to reduction in the number of preventable stillbirths. Regular facility-based stillbirth review meetings and healthcare provider accountability would also help to reduce the burden of this silent epidemic as well as reach the goal of a "single-digit" stillbirth rate by the year 2030.
Keywords: Classification of stillbirth; ReCoDe classification; Stillbirth.
© Federation of Obstetric & Gynecological Societies of India 2021.
Conflict of interest statement
Conflict of interestAll authors declare that they have no conflict of interest.
Figures
Similar articles
-
Classifying stillbirths in a tertiary care hospital of India: International Classification of Disease-perinatal Mortality (ICD-PM) versus cause of death-associated condition (CODAC) system.J Obstet Gynaecol. 2021 Feb;41(2):229-233. doi: 10.1080/01443615.2020.1736016. Epub 2020 Apr 29. J Obstet Gynaecol. 2021. PMID: 32347769
-
Using routine data to examine factors associated with stillbirth in three tertiary maternity facilities in Kabul, Afghanistan.Reprod Health. 2025 Jan 3;22(1):1. doi: 10.1186/s12978-024-01916-9. Reprod Health. 2025. PMID: 39754203 Free PMC article.
-
Identification of factors associated with stillbirth in the Indian state of Bihar using verbal autopsy: A population-based study.PLoS Med. 2017 Aug 1;14(8):e1002363. doi: 10.1371/journal.pmed.1002363. eCollection 2017 Aug. PLoS Med. 2017. PMID: 28763449 Free PMC article.
-
Making stillbirths visible: a systematic review of globally reported causes of stillbirth.BJOG. 2018 Jan;125(2):212-224. doi: 10.1111/1471-0528.14971. Epub 2017 Nov 29. BJOG. 2018. PMID: 29193794
-
Stillbirths in India: Current Status, Challenges, and the Way Forward.Indian J Pediatr. 2023 Dec;90(Suppl 1):63-70. doi: 10.1007/s12098-023-04807-2. Epub 2023 Aug 22. Indian J Pediatr. 2023. PMID: 37605065 Review.
References
LinkOut - more resources
Full Text Sources
Research Materials