

Case report of metastatic melanoma presenting as an unusual cause of gastrointestinal hemorrhage in an elderly gentleman
- PMID: 35734710
- PMCID: PMC9207090
- DOI: 10.1016/j.amsu.2022.103920
Case report of metastatic melanoma presenting as an unusual cause of gastrointestinal hemorrhage in an elderly gentleman
Abstract
Introduction: and Importance: Melanomas are capable of metastasizing to both regional and distant sites and are notably known to metastasize to the skin, lungs, brain, liver, bone, and gastrointestinal tract. Metastatic melanoma is infrequently diagnosed in vivo, and usually found only on post-mortem evaluation at autopsy.
Case presentation: Here we present the case of a 64-year-old male who originally presented with melena, fatigue, exertional dyspnea and one episode of near-syncope. He was found to have a hemoglobin of 5.4 gm/dL on initial presentation with largely unremarkable abdominal examination. CTAP demonstrated an area of circumferential small bowel wall thickening, concerning for malignancy. The patient underwent an EGD that was noted for mild gastric fundal erosions, which failed to explain his presenting symptoms. VCE was later performed following discharge to visualize the small bowel, which revealed two bleeding lesions within the small bowel. This was complicated by the device becoming lodged on the more proximal mass, and he was admitted again for push-enteroscopy and device retrieval. At the time of this admission, he continued to be symptomatic and was profoundly anemic with a hemoglobin of 4.7 gm/dL.
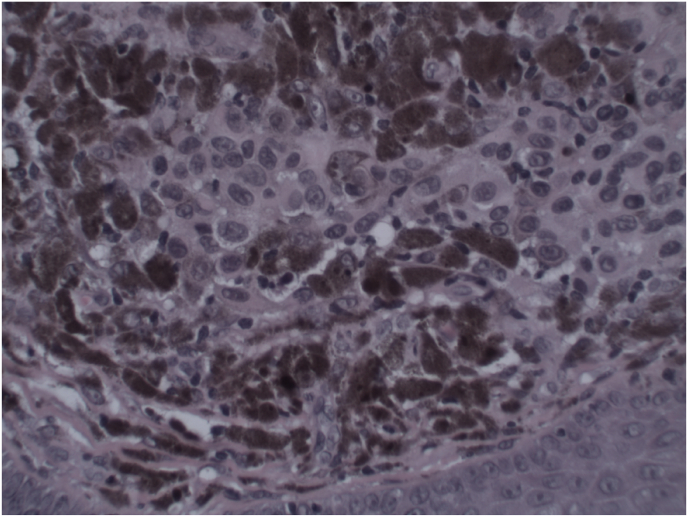
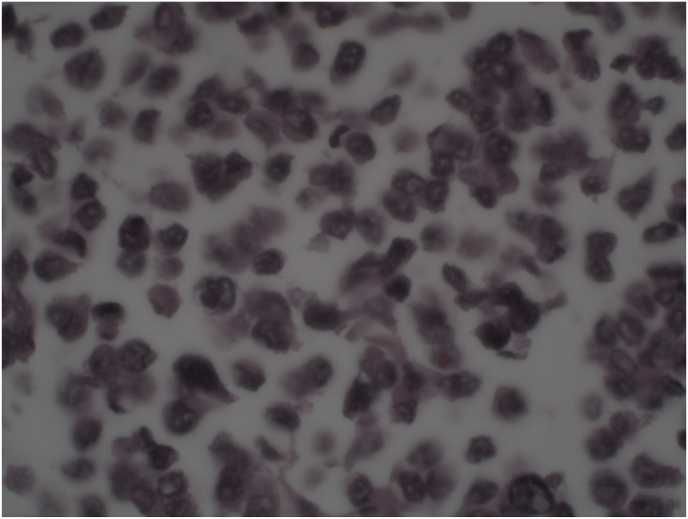
Clinical discussion: EGD with push enteroscopy was performed, revealing two small masses in the mid-distal duodenum and jejunum, which were tattooed and biopsied. He underwent robotic-assisted laparoscopic small bowel resection of the affected portions of the small bowel, without complications. Surgical samples were consistent with melanoma, and further dermatologic examination revealed a suspicious lesion located on the patient's posterior right shoulder was biopsied and also consistent with melanoma, confirming the suspicion for metastatic process from primary cutaneous lesion.
Conclusions: We present this case as a rare diagnostic opportunity to observe metastatic melanoma of the small bowel, including a review of pertinent symptomatology and epidemiological data from previous literature. Our case serves as a reminder to consider metastatic melanoma as a rather uncommon cause of severe blood loss anemia, while also providing an overview of endoscopic modalities available for visualizing the small bowel in the management of suspected small bowel malignancy.
Keywords: CT, computerized tomography; CTAP, computerized tomography of the abdomen and pelvis; EGD, esophogastroduodenoscopy; GI, gastrointestinal; HGB, hemoglobin; MCV, mean corpuscular volume; MM, metastatic melanoma; PET, positron emission tomography; RDW, red cell distribution width; VCE, video capsule endoscopy.
© 2022 The Authors.
Conflict of interest statement
No conflicts of interest.
Figures



Similar articles
-
Wandering Mucosal Melanoma Presenting as Occult Gastrointestinal Blood Loss Anemia.Cureus. 2022 Jun 2;14(6):e25614. doi: 10.7759/cureus.25614. eCollection 2022 Jun. Cureus. 2022. PMID: 35795509 Free PMC article.
-
Melanoma Metastasizing to the Small Intestine: A Case Report Illustrating Symptomatic and Asymptomatic Involvement.Cureus. 2016 May 13;8(5):e608. doi: 10.7759/cureus.608. Cureus. 2016. PMID: 27330876 Free PMC article.
-
An obscure cause of gastrointestinal bleeding: Renal cell carcinoma metastasis to the small bowel.Int J Surg Case Rep. 2015;15:130-2. doi: 10.1016/j.ijscr.2015.08.011. Epub 2015 Aug 13. Int J Surg Case Rep. 2015. PMID: 26348395 Free PMC article.
-
Metastatic melanoma to the gastrointestinal tract: role of surgery as palliative treatment.W V Med J. 2013 Jan-Feb;109(1):30-3. W V Med J. 2013. PMID: 23413546 Review.
-
The Usefulness of Capsule Endoscopy for Small Bowel Tumors.Clin Endosc. 2016 Jan;49(1):21-5. doi: 10.5946/ce.2016.49.1.21. Epub 2016 Jan 28. Clin Endosc. 2016. PMID: 26855919 Free PMC article. Review.
Cited by
-
Dysphagia in an 80-Year-Old Woman: A Rare Case of Metastatic Melanoma Presenting in the Small Bowel.Cureus. 2024 Oct 13;16(10):e71373. doi: 10.7759/cureus.71373. eCollection 2024 Oct. Cureus. 2024. PMID: 39534845 Free PMC article.
References
-
- Lens M., Bataille V., Krivokapic Z. Melanoma of the small intestine. Lancet Oncol. 2009;10(5):516–521. doi: 10.1016/S1470-2045(09)70036-1. https://www.ncbi.nlm.nih.gov/pubmed/19410196 - DOI - PubMed
-
- Amar A., Jougon J., Edouard A., Laban P., Marry J.P., Hillion G.P. Primary malignant melanoma of the small intestine. Gastroenterol. Clin. Biol. 1992;16:365–367. - PubMed
-
- Van Heukelom J.G., Gutnik S.H. The utility of video capsule endoscopy (VCE) for the detection of small bowel bleeding arising from benign and malignant tumors: report of two cases. S D Med. 2011;64(10) - PubMed
Publication types
LinkOut - more resources
Full Text Sources
