

Persistent left superior vena cava in a 29-year-old lady with Ebstein's anomaly and complete heart block. A case report and literature review
- PMID: 35734721
- PMCID: PMC9207079
- DOI: 10.1016/j.amsu.2022.103884
Persistent left superior vena cava in a 29-year-old lady with Ebstein's anomaly and complete heart block. A case report and literature review
Abstract
Introduction: Persistent Left Superior Vena Cava (PLSVC) is a rare congenital vascular anomaly that may occur alone or in combination with complex congenital heart anomalies and dangerous arrhythmias. We report the first case in the literature of combined PLSVC, Ebstein's Anomaly (Type A) and complete atrioventricular block in an adult female, being successfully managed with permanent pacemaker implantation in Sierra Leone.
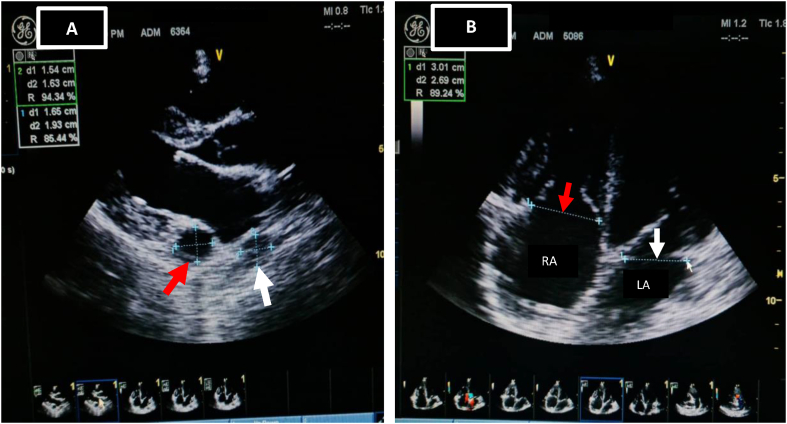
Case summary: We present an interesting case of a 29-year-old female, referred to the cardiology clinic on account of breathlessness, dizziness, and recurrent syncope. Physical examination revealed a pulse rate of 39 bpm, jugular venous pulse with occasional cannon waves, and grade 3/6 pansystolic murmur in the tricuspid valve area. An electrocardiogram confirmed complete atrioventricular block with junctional escape rhythm, while Transthoracic Echocardiogram (TTE) confirmed Ebstein's Anomaly (Type A) and moderate tricuspid regurgitation. PLSVC was discovered as an incidental intraprocedural finding. Deploying a pacemaker lead through this venous anomaly from the left side was futile. Nevertheless, we used a right sided approach that resulted in a successful permanent pacemaker implantation with optimal and stable parameters.
Conclusion: This rare case report highlights the practical challenges often encountered in the practice of cardiology during pacemaker and other cardiac device implantation. Cardiologists and critical care physicians should be acquainted with the venous anomaly of PLSVC, its variants, and procedure-associated risks, for better clinical decision making.
Keywords: Complete atrioventricular block; Ebstein anomaly; PLSVC; Permanent pacemaker.
© 2022 The Authors.
Conflict of interest statement
Authors of this article have no conflict or competing interests. Final version of the manuscript was approved by the authors.
Figures



Similar articles
-
Incidental Finding of a Persistent Left Superior Vena Cava During Permanent Dual-Chamber Pacemaker Implantation: A Case Report.Cureus. 2024 Nov 1;16(11):e72865. doi: 10.7759/cureus.72865. eCollection 2024 Nov. Cureus. 2024. PMID: 39493344 Free PMC article.
-
Two Cases of Cardiac Implantable Electronic Device Placement via Persistent Left Superior Vena Cava.Eur J Case Rep Intern Med. 2020 Mar 24;7(5):001484. doi: 10.12890/2020_001484. eCollection 2020. Eur J Case Rep Intern Med. 2020. PMID: 32399440 Free PMC article.
-
Permanent pacemaker implantation in a patient with persistent left superior vena cava with an absent right superior vena cava: A case report.J Cardiol Cases. 2020 Dec 11;24(1):34-36. doi: 10.1016/j.jccase.2020.11.024. eCollection 2021 Jul. J Cardiol Cases. 2020. PMID: 34257759 Free PMC article.
-
Persistent left superior vena cava with absent right superior vena cava: a case report and review of the literature.Cardiovasc J Afr. 2010 May-Jun;21(3):164-6. Cardiovasc J Afr. 2010. PMID: 20532458 Free PMC article. Review.
-
Persistent left superior vena cava: case report and literature review.Respir Care. 2000 Apr;45(4):411-6. Respir Care. 2000. PMID: 10780037 Review.
References
-
- Povoski S.P., Khabiri H. Persistent left superior vena cava: review of the literature, clinical implications, and relevance of alterations in thoracic central venous anatomy as pertaining to the general principles of central venous access device placement and venography in cancer patients. World J. Surg. Oncol. 2011;28:173. - PMC - PubMed
-
- Tak T., Crouch E., Drake G.B. Persistent left superior vena cava: incidence, significance and clinical correlates. Int. J. Cardiol. 2002;82(1):92–93. - PubMed
-
- Ruano C.A., Marinho-da-Silva A., Donato P. Congenital thoracic venous anomalies in adults: morphologic MR imaging. Curr. Probl. Diagn. Radiol. 2015;44(4):337–345. - PubMed
-
- Dearani J.A., Danielson G.K. Surgical management of Ebstein's anomaly in the adult. Semin. Thorac. Cardiovasc. Surg. 2005;17(2):148–154. - PubMed
-
- Carpentier A., Chauvaud S., Mace L., Relland J., Mihaileanu S., Marino J.P., Abry B., et al. A new reconstructive operation for Ebstein's anomaly of the tricuspid valve. J. Thorac. Cardiovasc. Surg. 1988;96:92–101. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
