

A standardized workflow for respiratory-gated motion management decision-making
- PMID: 35737295
- PMCID: PMC9359043
- DOI: 10.1002/acm2.13705
A standardized workflow for respiratory-gated motion management decision-making
Abstract
Purpose: Motion management of tumors within the lung and abdomen is challenging because it requires balancing tissue sparing with accuracy of hitting the target, while considering treatment delivery efficiency. Physicists can play an important role in analyzing four-dimensional computed tomography (4DCT) data to recommend the optimal respiratory gating parameters for a patient. The goal of this work was to develop a standardized procedure for making recommendations regarding gating parameters and planning margins for lung and gastrointestinal stereotactic body radiotherapy (SBRT) treatments. In doing so, we hoped to simplify decision-making and analysis, and provide a tool for troubleshooting complex cases.
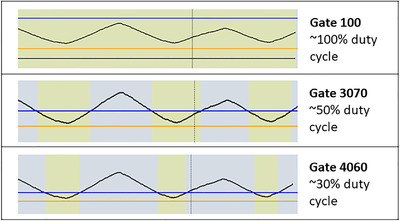
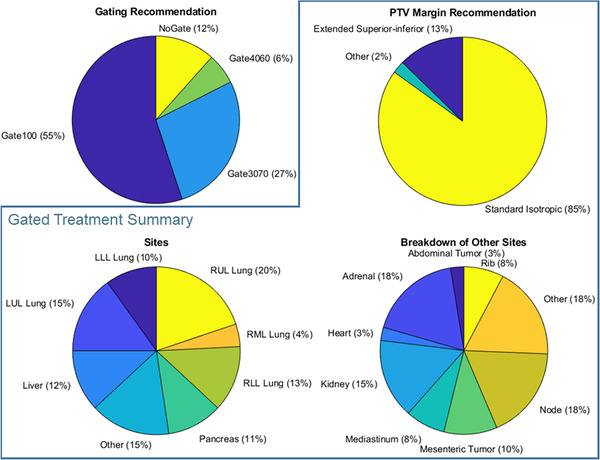
Methods: Factors that impact gating decisions and planning target volume (PTV) margins were identified. The gating options included gating on exhale with approximately a 50% duty cycle (Gate3070), exhale gating with a reduced duty cycle (Gate4060), and treating for most of respiration, excluding only extreme inhales and exhales (Gate100). A standard operating procedure was developed, as well as a physics consult document to communicate motion management recommendations to other members of the treatment team. This procedure was implemented clinically for 1 year and results are reported below.
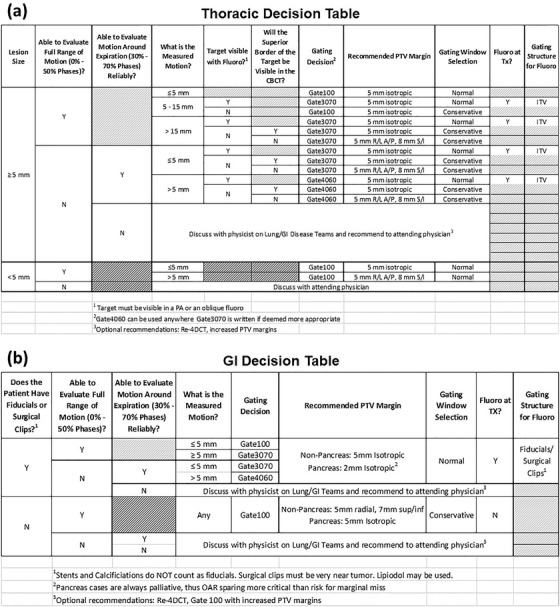
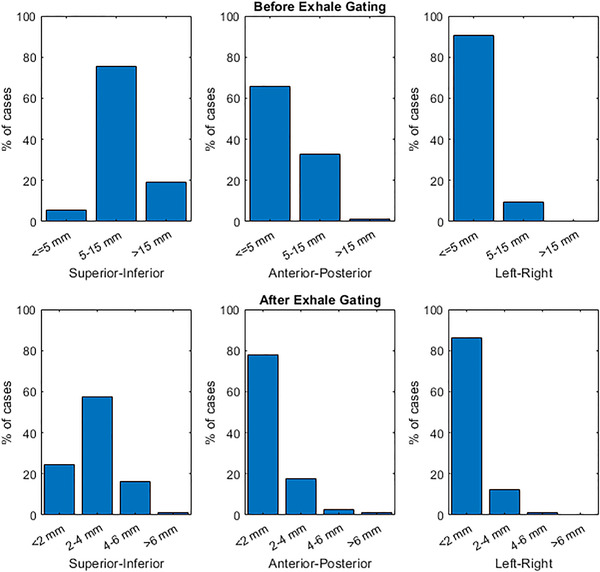
Results: Identified factors that impact motion management included the magnitude of motion observed on 4DCT, the regularity of breathing and quality of 4DCT data, and ability to observe the target on fluoroscopy. These were collated into two decision tables-one specific to lung tumors and another for gastrointestinal tumors-such that a physicist could answer a series of questions to determine the optimal gating and PTV margin. The procedure was used clinically for 252 sites from 213 patients treated with respiratory-gated SBRT and standardized practice across our 12-member physics team.
Conclusion: Implementation of a standardized procedure for respiratory gating had a positive impact in our clinic, improving efficiency and ease of 4DCT analysis and standardizing gating decision-making amongst physicists.
Keywords: gastrointestinal cancer; lung cancer; motion management; respiratory gating; stereotactic body radiotherapy.
© 2022 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, LLC on behalf of The American Association of Physicists in Medicine.
Conflict of interest statement
Kelly Kisling, Todd Atwood, and Xenia Ray acknowledge Honoraria and speaker fees from Varian Medical Systems. Xenia Ray has a research agreement with Varian Medical Systems.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
