

Efficacy of Ipilimumab vs FOLFOX in Combination With Nivolumab and Trastuzumab in Patients With Previously Untreated ERBB2-Positive Esophagogastric Adenocarcinoma: The AIO INTEGA Randomized Clinical Trial
- PMID: 35737383
- PMCID: PMC9227706
- DOI: 10.1001/jamaoncol.2022.2228
Efficacy of Ipilimumab vs FOLFOX in Combination With Nivolumab and Trastuzumab in Patients With Previously Untreated ERBB2-Positive Esophagogastric Adenocarcinoma: The AIO INTEGA Randomized Clinical Trial
Abstract
Importance: In metastatic esophagogastric adenocarcinoma (EGA), the addition of programmed cell death 1 (PD-1) inhibitors to chemotherapy has improved outcomes in selected patient populations.
Objective: To investigate the efficacy of trastuzumab and PD-1 inhibitors with cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) inhibitors or FOLFOX in first-line treatment of advanced ERBB2-positive EGA.
Design, setting, and participants: This phase 2 multicenter, outpatient, randomized clinical trial with 2 experimental arms compared with historical control individually was conducted between March 2018 and May 2020 across 21 German sites. The reported results are based on a median follow-up of 14.3 months. Patients with previously untreated, metastatic ERBB2-positive (local immunohistochemistry score of 3+ or 2+/in situ hybridization amplification positive) EGA, adequate organ function, and eligibility for immunotherapy were included. Data analysis was performed from June to September 2021.
Interventions: Patients were randomized to trastuzumab and nivolumab (1 mg/kg × 4/240 mg for up to 12 months) in combination with mFOLFOX6 (FOLFOX arm) or ipilimumab (3 mg/kg × 4 for up to 12 weeks) (ipilimumab arm).
Main outcomes and measures: The primary end point was survival improvement with a targeted increase of the 12-month overall survival rate from 55% (trastuzumab/chemotherapy-ToGA regimen) to 70% in each arm.
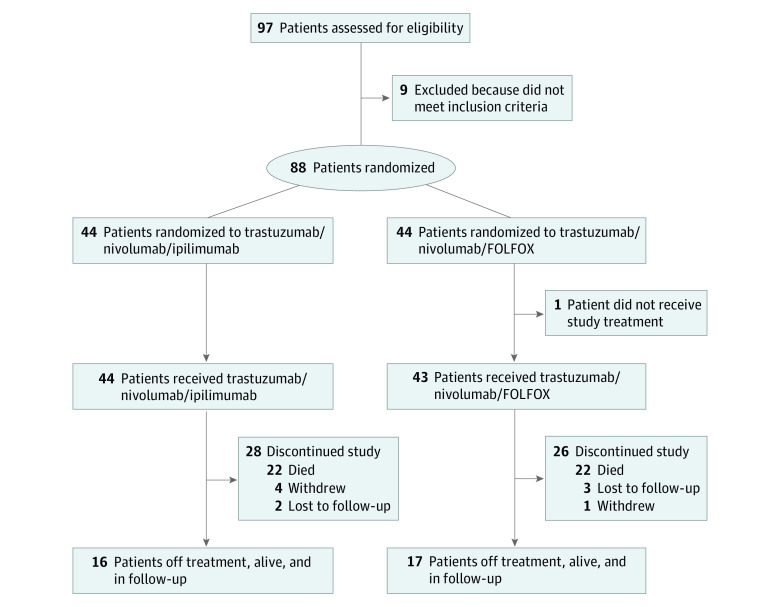
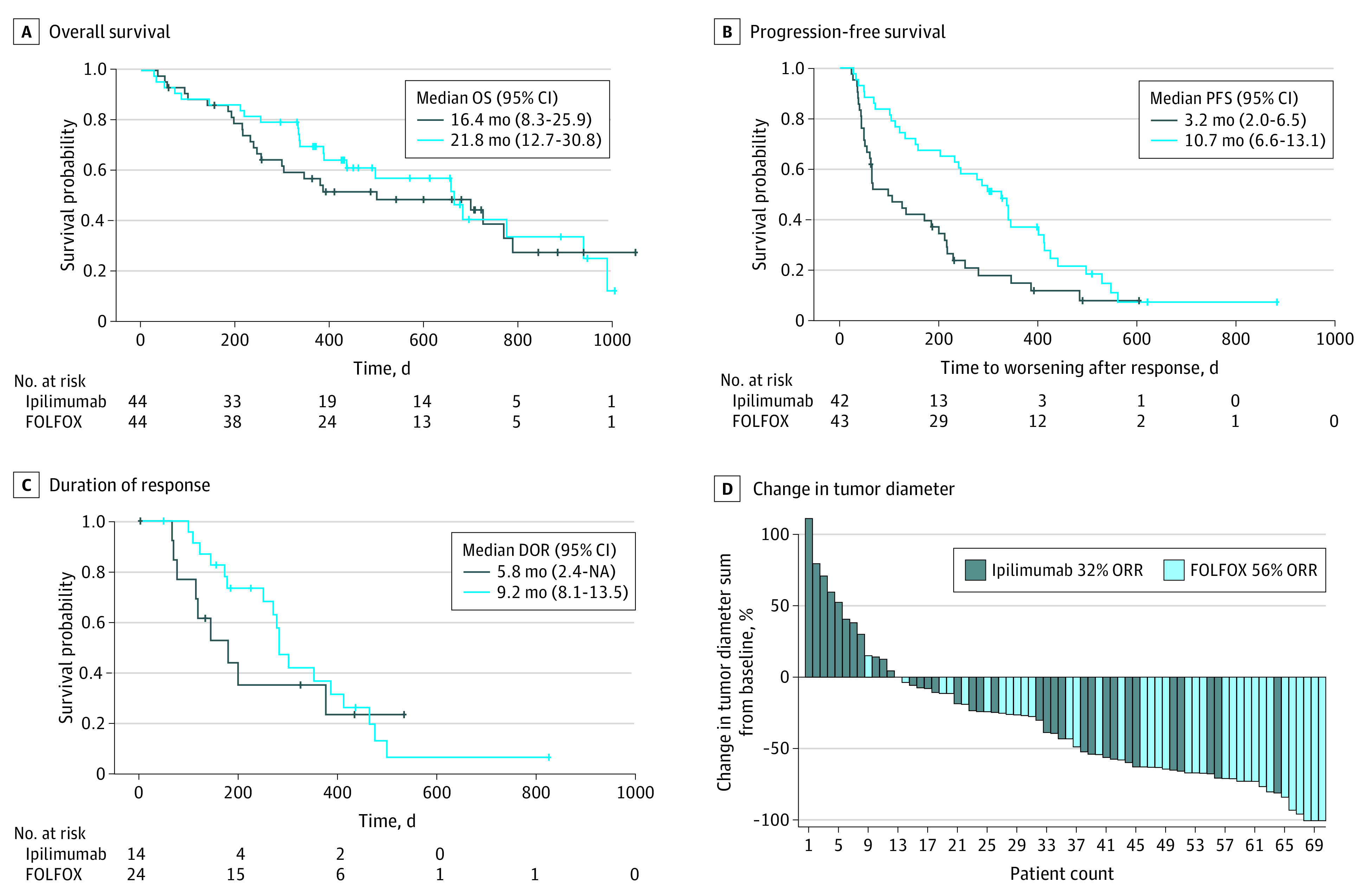
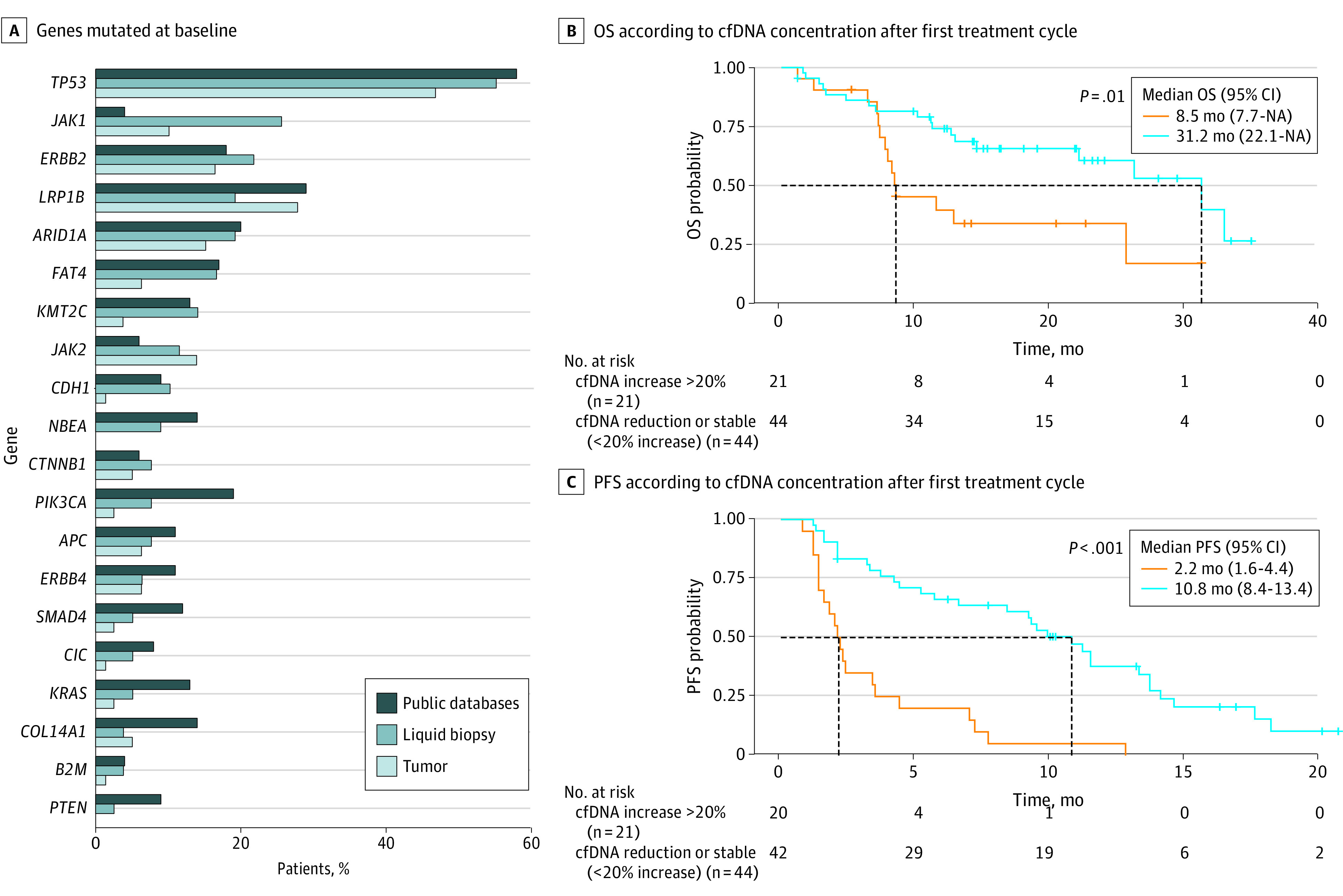
Results: A total of 97 patients were enrolled, and 88 were randomized (18 women, 70 men; median [range] age, 61 [41-80] years). Baseline Eastern Cooperative Oncology Group performance status was 0 in 54 patients (61%) and 1 in 34 patients (39%); 66 patients (75%) had EGA localized in the esophagogastric junction and 22 in the stomach (25%). Central post hoc biomarker analysis (84 patients) showed PD-1 ligand 1 (PD-L1) combined positive score of 1 or greater in 59 patients (72%) and 5 or greater in 46 patients (56%) and confirmed ERBB2 positivity in 76 patients. The observed overall survival rate at 12 months was 70% (95% CI, 54%-81%) with FOLFOX and 57% (95% CI, 41%-71%) with ipilimumab. Treatment-related grade 3 or greater adverse events (AEs) and serious AEs occurred in 29 and 15 patients in the FOLFOX arm and in 20 and 17 patients in the ipilimumab arm, respectively, with a higher incidence of autoimmune-related AEs in the ipilimumab arm and neuropathy in the FOLFOX arm. Liquid biopsy analyses showed strong correlation of early cell-free DNA increase with shorter progression-free and overall survival and emergence of truncating and epitope-loss ERBB2 resistance sequence variations with trastuzumab treatment.
Conclusions and relevance: In this randomized clinical trial, trastuzumab, nivolumab, and FOLFOX showed favorable efficacy compared with historical data and trastuzumab, nivolumab, and ipilimumab in ERBB2-positive EGA. The ipilimumab arm yielded similar OS compared with the ToGA regimen.
Trial registration: ClinicalTrials.gov Identifier: NCT03409848.
Conflict of interest statement
Figures
Comment in
-
AIO INTEGA Provides Further Support for Immunotherapy in Patients With Advanced ERBB2-Positive Gastroesophageal Adenocarcinoma.JAMA Oncol. 2022 Aug 1;8(8):1158-1159. doi: 10.1001/jamaoncol.2022.2008. JAMA Oncol. 2022. PMID: 35737402 No abstract available.
References
-
- Bang YJ, Van Cutsem E, Feyereislova A, et al. ; ToGA Trial Investigators . Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687-697. doi:10.1016/S0140-6736(10)61121-X - DOI - PubMed
-
- Tabernero J, Hoff PM, Shen L, et al. . Pertuzumab plus trastuzumab and chemotherapy for HER2-positive metastatic gastric or gastro-oesophageal junction cancer (JACOB): final analysis of a double-blind, randomised, placebo-controlled phase 3 study. Lancet Oncol. 2018;19(10):1372-1384. doi:10.1016/S1470-2045(18)30481-9 - DOI - PubMed
-
- Janjigian YY, Shitara K, Moehler M, et al. . First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet. 2021;398(10294):27-40. doi:10.1016/S0140-6736(21)00797-2 - DOI - PMC - PubMed
-
- Sun JM, Shen L, Shah MA, et al. ; KEYNOTE-590 Investigators . Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet. 2021;398(10302):759-771. doi:10.1016/S0140-6736(21)01234-4 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
