

Cost-effectiveness analysis of semaglutide 2.4 mg for the treatment of adult patients with overweight and obesity in the United States
- PMID: 35737858
- PMCID: PMC10372962
- DOI: 10.18553/jmcp.2022.28.7.740
Cost-effectiveness analysis of semaglutide 2.4 mg for the treatment of adult patients with overweight and obesity in the United States
Abstract
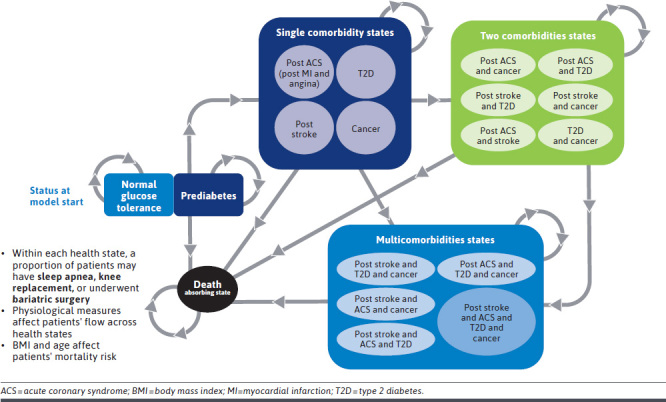
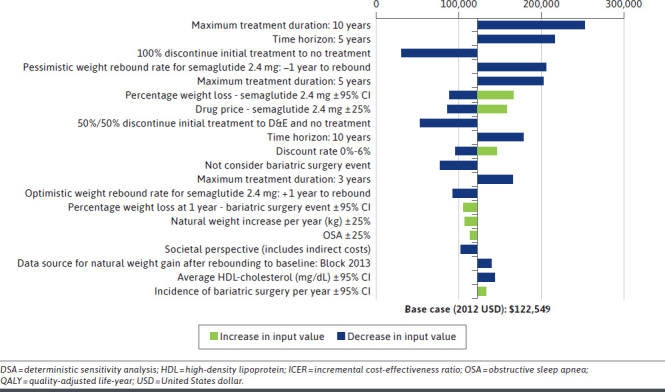
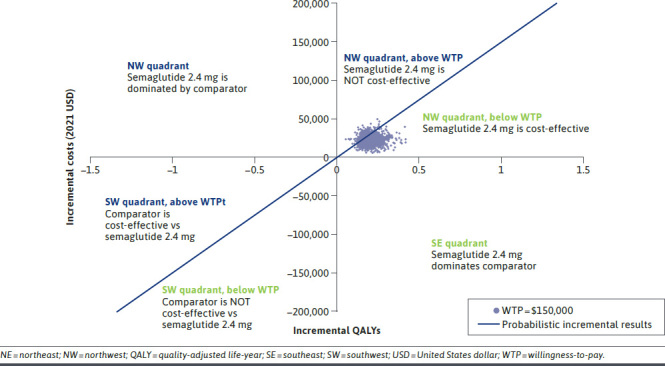
BACKGROUND: The rising prevalence and associated public health burden of obesity has led to advancements in pharmaceuticals for weight management. Semaglutide 2.4 mg, an anti-obesity medication (AOM) recently approved by the US Food and Drug Administration, has demonstrated clinically relevant weight loss in its phase 3 clinical trials. Economic evaluation comparing semaglutide 2.4 mg with other available weight management therapies is essential to inform payers for decision-making. OBJECTIVES: To assess the cost-effectiveness of semaglutide 2.4 mg in the treatment of adult patients with obesity (ie, body mass index [BMI] ≥ 30) and adult patients who are overweight (ie, BMI 27-29.9) with 1 or more weight-related comorbidities from a US third-party payer perspective. METHODS: A cohort Markov model was constructed to compare semaglutide 2.4 mg with the following comparators: no treatment, diet and exercise (D&E), and 3 branded AOMs (liraglutide 3 mg, phentermine-topiramate, and naltrexone-bupropion). All AOMs, including semaglutide 2.4 mg, were assumed to be taken in conjunction with D&E. Changes in BMI, blood pressure, cholesterol level, experience of acute and chronic obesity-related complications, costs, and quality-adjusted life years (QALYs) were simulated over 30 years based on pivotal trials of the AOMs and other relevant literature. Drug and health care prices reflect 2021 standardized values. Cost-effectiveness was examined with a willingness-to-pay (WTP) threshold of $150,000 per QALY gained. Sensitivity analyses were conducted to test the robustness of the cost-effectiveness results to plausible variation in model inputs. RESULTS: In the base-case analysis, treatment with semaglutide 2.4 mg was estimated to improve QALYs by 0.138 to 0.925 and incur higher costs by $3,254 to $25,086 over the 30-year time horizon vs comparators. Semaglutide 2.4 mg is cost-effective against all comparators at the prespecified WTP threshold, with the incremental cost per QALY gained ranging from $23,556 to $144,296 per QALY gained. In the sensitivity analysis, extended maximum treatment duration, types of subsequent treatment following therapy discontinuation, and weight-rebound rates were identified as key drivers for model results. The estimated probability of semaglutide 2.4 mg being cost-effective compared with comparators ranged from 67% to 100% when varying model parameters and assumptions. CONCLUSIONS: As a long-term weight management therapy, semaglutide 2.4 mg was estimated to be cost-effective compared with no treatment, D&E alone, and all other branded AOM comparators under a WTP threshold of $150,000 per QALY gained over a 30-year time horizon. DISCLOSURES: Financial support for this research was provided by Novo Nordisk Inc. The study sponsor was involved in several aspects of the research, including the study design, the interpretation of data, the writing of the manuscript, and the decision to submit the manuscript for publication. Dr Kim and Ms Ramasamy are employees of Novo Nordisk Inc. Ms Kumar and Dr Burudpakdee were employees of Novo Nordisk Inc at the time this study was conducted. Dr Sullivan received research support from Novo Nordisk Inc for this study. Drs Wang, Song, Wu, Ms Xie, and Ms Sun are employees of Analysis Group, Inc, who received consultancy fees from Novo Nordisk Inc in connection with this study.
Conflict of interest statement
Financial support for this research was provided by Novo Nordisk Inc. The study sponsor was involved in several aspects of the research, including the study design, the interpretation of data, the writing of the manuscript, and the decision to submit the manuscript for publication.
Dr Kim and Ms Ramasamy are employees of Novo Nordisk Inc. Ms Kumar and Dr Burudpakdee were employees of Novo Nordisk Inc at the time this study was conducted. Dr Sullivan received research support from Novo Nordisk Inc for this study. Drs Wang, Song, Wu, Ms Xie, and Ms Sun are employees of Analysis Group, Inc, who received consultancy fees from Novo Nordisk Inc in connection with this study.
Figures
References
-
- Centers for Disease Control and Prevention. Overweight and obesity: Adult obesity facts. 2021. Accessed May 21, 2021. https://www.cdc.gov/obesity/data/adult.html
-
- Fryar C, Carroll M, Afful J. Prevalence of overweight, obesity, and severe obesity among adults aged 20 and over: United States, 1960–1962 Through 2017–2018. 2021. https://www.cdc.gov/nchs/data/hestat/obesity-adult-17-18/obesity-adult.h...
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
